TO: Administrative File: CAG-00067R2
FROM: Tamara Syrek Jensen, JD
Director, Coverage and Analysis Group
Joseph Chin, MD, MS
Deputy Director, Coverage and Analysis Group
Lori Ashby, MA
Director, Division of Policy and Evidence Review
Rosemarie Hakim, PhD
Acting Director, Evidence Development Division
Joseph Hutter, MD, MA
Medical Officer
Carl Li, MD, MPH
Medical Officer
Stuart Caplan, RN, MAS
Lead Analyst
Ruth McKesson
Analyst
SUBJECT: National Coverage Determination for Ambulatory Blood Pressure Monitoring
DATE: July 2, 2019
I. Decision
- The Centers for Medicare & Medicaid Services (CMS) has determined that the evidence is sufficient to cover ambulatory blood pressure monitoring (ABPM) for the diagnosis of hypertension in Medicare beneficiaries under the following circumstances:
- For beneficiaries with suspected white coat hypertension, which is defined as an average office blood pressure of systolic blood pressure greater than 130 mm Hg but less than 160 mm Hg or diastolic blood pressure greater than 80 mm Hg but less than 100 mm Hg on two separate clinic/office visits with at least two separate measurements made at each visit and with at least two blood pressure measurements taken outside the office which are <130/80 mm Hg.
- For beneficiaries with suspected masked hypertension, which is defined as average office blood pressure between 120 mm Hg and 129 mm Hg for systolic blood pressure or between 75 mm Hg and 79 mm Hg for diastolic blood pressure on two separate clinic/office visits with at least two separate measurements made at each visit and with at least two blood pressure measurements taken outside the office which are ≥130/80 mm Hg.
ABPM devices must be:
- capable of producing standardized plots of blood pressure measurements for 24 hours with daytime and night-time windows and normal blood pressure bands demarcated;
- provided to patients with oral and written instructions and a test run in the physician’s office must be performed; and
- interpreted by the treating physician or treating non-physician practitioner.
For eligible patients, ABPM is covered once per year.
- Coverage of other indications for ABPM are at the discretion of the Medicare Administrative Contractors.
See Appendix B for the manual language.
II. Background
Throughout this document we use numerous acronyms, some of which are not defined as they are presented in direct quotations. Please find below a list of these acronyms and corresponding full terminology:
ABPM – Ambulatory Blood Pressure Monitoring
ACC – American College of Cardiology
AHA – American Heart Association
APWV - Aortic Pulse Wave Velocity
BMI – Body Mass Index
BP – Blood Pressure
CDC: Centers for Disease Control and Prevention
CHAP - Cardiovascular Health Awareness Program
CI – Confidence Interval
CIM – Coverage Issues Manual
CINAHL – Cumulative Index to Nursing and Allied Health Literature
CMS – Centers for Medicare & Medicaid Services
CKD – Chronic Kidney Disease
COR – Class of Recommendation
CV – Cardiovascular
CVD – Cardiovascular Disease
DBP – Diastolic Blood Pressure
DHS – Dallas Heart Study
ENRICA – Spanish Nutrition and Cardiovascular Risk Survey
FDA – Food and Drug Administration
GFR – Glomerular Filtration Rate
HF – Heart Failure
HR – Hazard Ratio
IDACO – International Database on Ambulatory Blood Pressure Monitoring in Relation to Cardiovascular Outcomes
IHD – Ischemic Heart Disease
JNC 7 – The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
JNC 8 – The Eighth Joint National Committee Guidelines and the Outpatient Management of Hypertension in the African-American Population
LOE – Level of Evidence
MES – Multi-Ethnic Study of Atherosclerosis
MetS - metabolic syndrome
MI – Myocardial Infarction
mm Hg – Millimeters of Mercury
NCA – National Coverage Analysis
NCD –National Coverage Determination
NHANES – National Health and Nutrition Examination Study
NOS - Newcastle–Ottawa Quality Assessment Scale
NT - Normotensive
OBPM – Office Blood Pressure Monitoring
OR – Odds Ratio
PAMELA – Pressioni Arteriose Monitorate E Loro
RR – Relative Risk
SBP – Systolic Blood Pressure
SD – Standard Deviation
SPRINT – Systolic Blood Pressure Intervention Trial
TA – Technology Assessment
The Act – Social Security Act
US –United States
USPSTF – United States Preventive Services Task Force
WCE – White Coat Effect
WCH –White Coat Hypertension
What is hypertension (high blood pressure)?
The American Heart Association (AHA) defines blood pressure as a force that pushes blood through a network of arteries, veins and capillaries. The blood pressure reading is the result of two forces: the systolic pressure occurs as blood pumps out of the heart and into the arteries; diastolic pressure is created as the heart rests between heart beats (American Heart Association, 2018). Elevated blood pressure, or hypertension, leads to harm by causing tiny tears in the interior lining (intima) of the arteries and coronary vessels, stimulating a local immune response in the endothelial cells within the atrial walls. In these regions, the arterial intima retains apolipoprotein B, which attracts lipid-rich macrophages (foam cells). These preatherotic lesions develop into atherosclerotic plaques which become increasingly fibrotic and can form fissures, hematomas, thrombi, and calcifications (Swirski and Nahrendorf, 2013). The end result is stiff, thickened arteries that narrow the flow of blood to organs and limbs, which both increases pressure on target organs and limits oxygenation of them.
There is also the risk of atherosclerotic plaque rupture, resulting in distal vascular obstruction and ischemia and infarction of end organs, such as stroke in the brain (U.S. Department of Health & Human Services, 2018).
Population based risks of hypertension
Global: According to a systematic analysis for the Global Burden of Disease Study 2010, hypertension was the number one risk factor for death, responsible for approximately 9.4 million deaths globally from cardiac disease, including ischemic disease and heart failure, cerebrovascular disease, peripheral vascular disease, aortic disease, and kidney disease in that year (Lim et al., 2012). Another global systematic analysis based on 844 studies from 154 countries estimated that the rate of elevated SBP increased substantially between 1990 and 2015, and deaths associated with elevated SBP also increased (Forouzanfar, et al., 2017). Projections based on this sample suggested that in 2015, an estimated 3.5 billion adults had SBP of at least 110 to 115 mmHg and 874 million adults had SBP of 140 mm Hg or higher.
United States: In the 2013-2016 National Health and Nutrition Examination Survey (NHANES), the prevalence of hypertension (defined at that time as SBP ≥140 or DBP ≥90) in the US was 30.5% (CDC, 2017). The rate of uncontrolled hypertension among known hypertensives was 55.4%. Hypertension was somewhat more prevalent in men than women (31.5% vs. 29.3%, respectively), but men were much more likely to have uncontrolled hypertension (60.9% vs. 46.7%). Blacks had a higher prevalence of hypertension than whites, Latinos, or Asians (42.4%, 29.2%, 29%, and 27%, respectively). By age, 67.4% of women 65–74 years and 78.7% of women 75 years and older had hypertension. Among men, the prevalence was 61.1% and 67.4%, respectively (CDC, 2016).
Impact of hypertension on patient outcomes
Mortality, stroke and cardiovascular disease
An analysis of US data from nationally representative health surveys and disease-specific mortality statistics reported that about 1 in 5 deaths in the US were attributable to hypertension (Danaei et al., 2009). The US mortality rate decreased among hypertensive adults between the 1970s and 1990s, but the mortality gap between adults with and without hypertension remained relatively constant (Ford et al., 2011).
In a pooled meta-analysis of individual data on nearly one million adults in 61 prospective cohorts from Europe, Japan, North America, Australia and China, researchers found that the risk of death from stroke, ischemic heart disease (IHD), and other vascular causes increased from SBP levels <115 mm Hg to >180 mm Hg and from DBP levels <75 mm Hg to >105 mm Hg (Lewington et al., 2002). In that analysis, at ages 40–69 years, each difference of 20 mm Hg usual SBP (or, approximately equivalently, 10 mm Hg usual DBP) was associated with more than a twofold difference in the stroke death rate, and with twofold differences in the death rates from IHD and from other vascular causes.
A second study of more than one million UK individuals followed for a mean of 5 years found more specific relationships between elevated BP and cardiovascular disease (Rapsomaniki, et al., 2014). At every age increment the lowest risk for cardiovascular disease was in people with systolic blood pressure of 90–114 mm Hg and diastolic blood pressure of 60–74 mm Hg, with no evidence of a J-shaped increased risk at lower blood pressures. The effect of high blood pressure varied by cardiovascular disease endpoint from strongly positive to no effect. Associations with high systolic blood pressure were strongest for intracerebral and subarachnoid hemorrhage (stroke), and stable angina; and weakest for abdominal aortic aneurysm. Elevated systolic blood pressure had a greater effect on angina, myocardial infarction, and peripheral arterial disease, while elevated diastolic blood pressure had a greater effect on abdominal aortic aneurysm. People with hypertension (defined as BP ≥140/90 mm Hg or those on BP lowering drugs) had a lifetime risk of cardiovascular disease at age 30 years of 63% compared with 46% for those with normal blood pressure, and developed cardiovascular disease 5 years earlier.
Kidney disease
Hypertension is the second leading cause of kidney failure. The nephrons in the kidneys are supplied with a dense network of blood vessels and high volumes of blood flow through them. Over time uncontrolled high blood pressure can cause arteries around the kidneys to narrow, weaken or harden.
These damaged arteries are not able to deliver enough blood to the kidney tissue. Kidney damage and uncontrolled high blood pressure affect aldosterone production contributing to a negative spiral of increasing blood pressure and eventual kidney failure.
Current definition and prevalence of hypertension
The 2001 ABPM NCD (See Appendix C) was based on the existing definitions of BP > 140/90 mm Hg. The 2017 American College of Cardiology/American Heart Association Task Force guidelines revised that definition as follows (Table 1) (Whelton et al., 2017). This will be discussed further in the evidence section.
| Table 1. Categories of BP in Adults* |
|---|
| BP Category |
SBP |
|
DBP |
| Normal |
<120 mm Hg |
and |
<80 mm Hg |
| Elevated |
120–129 mm Hg |
and |
<80 mm Hg |
Hypertension |
|
|
|
| Stage 1 |
130–139 mm Hg |
or |
80–89 mm Hg |
| Stage 2 |
≥140 mm Hg |
or |
≥90 mm Hg |
| *Individuals with SBP and DBP in 2 categories should be designated to the higher BP category. |
This definition differs from that previously recommended in the JNC 7 report, with stage 1 hypertension now defined as an SBP of 130–139 or a DBP of 80–89 mm Hg, and with stage 2 hypertension in the present document corresponding to stages 1 and 2 in the JNC 7 report (Chobanian et al., 2003). This new definition (Table 2) effectively increases the population prevalence of hypertension (based on reported antihypertensive medication use) from 64% and 63% of men and women ages 64-74 years, respectively, to 77% and 75%; and from 71% and 78% in men and women ages 75 years and older, respectively, to 79% and 85% (Whelton et al., 2017).
| Table 2 Prevalence of Hypertension Based on 2 SBP/DBP Thresholds*† |
|
SBP/DBP ≥130/80 mm Hg or Self- Reported Antihypertensive Medication† |
SBP/DBP ≥140/90 mm Hg or Self- Reported Antihypertensive Medication‡ |
| Overall, crude |
46% |
32% |
| |
Men |
Women |
Men |
Women |
| Overall, age-sex adjusted |
48% |
43% |
31% |
32% |
| Age group, y |
| 20–44 |
30% |
19% |
11% |
10% |
| 45–54 |
50% |
44% |
33% |
27% |
| 55–64 |
70% |
63% |
53% |
52% |
| 65–74 |
77% |
75% |
64% |
63% |
| 75+ |
79% |
85% |
71% |
78% |
| Race-ethnicity § |
| Non-Hispanic white |
47% |
41% |
31% |
30% |
| Non-Hispanic black |
59% |
56% |
42% |
46% |
| Non-Hispanic Asian |
45% |
36% |
29% |
27% |
| Hispanic |
44% |
42% |
27% |
32% |
| *130/80 and 140/90 mm Hg in 9623 participants (≥20 years of age) in NHANES 2011–2014.
†BP cutpoints for definition of hypertension in the present guideline.
‡BP cutpoints for definition of hypertension in JNC 7.
§ Adjusted to the 2010 age-sex distribution of the U.S. adult population.
BP indicates blood pressure; DBP, diastolic blood pressure; NHANES, National Health and Nutrition Examination Survey;
and SBP, systolic blood pressure |
*130/80 and 140/90 mm Hg in 9623 participants (≥20 years of age) in NHANES 2011–2014.
†BP cutpoints for definition of hypertension in the present guideline.
‡BP cutpoints for definition of hypertension in JNC 7.
§Adjusted to the 2010 age-sex distribution of the U.S. adult population.
BP indicates blood pressure; DBP, diastolic blood pressure; NHANES, National Health and Nutrition Examination Survey; and SBP, systolic blood pressure
Effectiveness of treatment for high blood pressure
There is solid evidence that pharmacologic interventions lower BP (Law et al, 2009) and that this in turn lowers the risk of cardiovascular disease. A recent meta-analysis combined 123 RCTs of BP- lowering treatment with more than 600,000 participants. The meta-regression showed reductions in the relative risk of cardiovascular disease proportional to the magnitude of the SBP reduction (Ettehad et al., 2016). Every 10 mm Hg reduction in systolic blood pressure significantly reduced the risk of major cardiovascular disease events (relative risk 0.80, 95% CI 0.77–0.83), coronary heart disease (0.83, 0.78–0·88), stroke (0.73, 0.68–0.77), and heart failure (0.72, 0.67–0.78), which, in the populations studied, led to a significant 13% reduction in all-cause mortality (0.87, 0.84–0.91). The Sprint MIND study, which measured the effect of intensive vs standard BP control on probable dementia, found that intensive BP control significantly reduced the risk of mild cognitive impairment (14.6 vs 18.3 cases/1000 person-years; HR 0.81; 95% CI 0.69-0.95) and the combined rate of mild cognitive impairment or probable dementia (20.2 vs 24.1 cases/1000 person-years; HR 0.85; 95% CI 0.74-0.97) (Williamson et al., 2019).
White coat hypertension and the white coat effect
White coat hypertension is defined as having a higher office BP (OBPM) than out-of-office BP (Whelton et al., 2017) among patients not being treated for high BP. Gorostidi, et al. (2015) defines WCH as an elevated office BP and a 24-h ambulatory BP of <130/80 mm Hg. The white coat effect (WCE) is defined as the transient blood pressure rise associated with the presence of a doctor (Verdecchia et al., 2002) among patients regardless of treatment. The true prevalence of white coat hypertension (WCH) is unknown in the US and reported prevalence figures vary by definition and composition of the population (Whelton et al., 2017). The likelihood of WCH increases with age, is more prevalent among males, and may be accompanied by diabetes and a history of prior cardiovascular events. WCH is not benign and a number of population based cohort studies have shown it to be related to incident metabolic syndrome and higher long term mortality and cardiovascular endpoints than normotensive controls (Tientcheu et al., 2015; Franklin et al., 2016; Huang et al., 2017; Banegas et al., 2018; Cuspidi et al., 2018).
Masked hypertension
Masked hypertension occurs when individuals with office based BP <130/80 mm Hg and have elevated ambulatory BP ≥130/80 (Whelton et al., 2017). It is estimated that 12.3% of adults and 28% of persons older than 65 years have masked hypertension (Wang et al., 2017). It is more prevalent in men and African Americans, increases with age and may be accompanied by diabetes. Like WCH, masked hypertension is associated with incident metabolic syndrome, long term mortality, and cardiovascular endpoints than normotensive controls (Tientcheu et al., 2015; Whelton et al., 2017; Banegas et al., 2018; Cuspidi et al., 2018).
Blood pressure measurement
Manual BP monitoring in the clinical office gives point-in-time BP readings. The most traditional method of measurement is the auscultatory method, in which a trained observer uses a stethoscope to detect Korotkoff sounds which are made by the turbulent flow of blood through the brachial artery past the restricted area created by the inflated cuff. The readings are made using a mercury or aneroid sphygmomanometer. Sources of observer error and bias in the auscultatory method include differences in auditory acuity and terminal digit rounding (Piper et al., 2014). Oscillometric sphygmomanometers use a pressure transducer to assess the oscillations of pressure in a cuff during gradual deflation. The point of maximum oscillation corresponds to the mean intra-arterial pressure. Systolic and diastolic measurements are then calculated based on an empirically derived algorithm (Piper et al., 2014).
Although the auscultatory methods are inherently accurate, they are dependent on attention to detail, which may be lacking, and they provide only a momentary measurement of BP under circumstances that can influence the level of BP being measured (O’Brien et al., 2013). Blood pressure can be measured by patients at home or in other environments. A small body of evidence suggests, but does not confirm, that home blood pressure monitoring may predict patient outcomes (Piper et al, 2014). Whelton et al (2017) stated that home BP measurement maybe a more practical approach in clinical practice. It should be noted that patient used home BP readings are generally not accurate when compared to standardized mercury sphygmomanometry (Ringrose et al, 2017).
ABPM devices provide a larger number of readings than OBPM and a profile of blood pressure in the patient’s usual environment. ABPM is intended to allow identification of white coat and masked hypertension, uncover nocturnal hypertension, and assess blood pressure variability over a 24-hour period as well as the 24-hour efficacy of antihypertensive medication (O’Brien et al, 2013).
ABPM devices are small portable machines connected to a BP cuff worn by patients that record BP at regular intervals over 24 to 48 hours while patients go about their normal activities, including sleep. Measurements are typically taken at 20- to 30-minute intervals. Results may be reported for 24 hours, daytime (awake), and nighttime (asleep). Modern ambulatory devices use oscillometric techniques (Piper et al., 2014).
The U.S. Preventive Services Task Force (USPSTF) recommends annual screening for high BP in adults aged 18 years or older and recommends obtaining measurements outside of the clinical setting (either ABPM or home BP monitoring) for diagnostic confirmation of high BP before starting treatment (Sui, 2015). The USPSTF specifically states that "In addition to office blood pressure measurement, ABPM and HBPM may be used to confirm a diagnosis of hypertension after initial screening" (US Preventive Services Task Force, 2019).
III. History of Medicare Coverage
CMS has covered ABPM since 2001 only for those patients with documented suspected white coat hypertension. On January 16, 2003, a technical correction for this NCD was issued to clarify that a physician is required to perform the interpretation of the data obtained through ABPM, but that there are no requirements regarding the setting in which the interpretation is performed.
A. Current Request
CMS received a complete, formal request for a reconsideration of the national coverage determination from the American Heart Association and American Medical Association. The formal request letter can be viewed on the tracking sheet for this NCA on the CMS website by clicking here.
B. Benefit Category
Medicare is a defined benefit program. For an item or service to be covered by the Medicare program, it must fall within one of the statutorily defined benefit categories outlined in the Social Security Act. ABPM may be considered to be within the benefits described under sections: other diagnostic tests §1861(s)(3).
Medicare regulations at 42 CFR 410.32(a) state in part, that "…diagnostic tests must be ordered by the physician who is treating the beneficiary, that is, the physician who furnishes a consultation or treats a beneficiary for a specific medical problem and who uses the results in the management of the beneficiary’s specific medical problem."
IV. Timeline of Recent Activities
| Date |
Action |
| October 9, 2018 | CMS posts a tracking sheet announcing the opening of an NCA. The initial 30- day public comment period begins. |
| November 8, 2018 | First public comment period ends. CMS receives 103 comments. |
| April 9, 2019 | Proposed Decision Memorandum posted. 30-day public comment period begins. |
V. Food and Drug Administration (FDA) Status
Companies manufacturing devices intended for 24 Hour, Ambulatory Blood Pressure monitoring have obtained clearance for marketing of these devices under the Food and Drug Administration’s (FDA) 510(k) process. The FDA considers all BP Monitoring devices to be Class II devices. All Ambulatory Blood Pressure monitors with FDA clearance have demonstrated accuracy compared to reference blood pressure measurements.
VI. General Methodological Principles
In general, when making national coverage determinations under section 1862(a)(1) of the Social Security Act, CMS evaluates relevant clinical evidence to determine whether or not the evidence is of sufficient quality to support a finding that an item or service falling within one or more benefit categories is reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member (§ 1862 (a)(1)(A)).
The critical appraisal of the evidence during a national coverage analysis enables us to determine to what degree we are confident that: 1) the specific assessment of a clinical question relevant to the coverage request can be answered conclusively; and 2) the intervention will improve health outcomes for beneficiaries. An improved health outcome is one of several considerations in determining whether an item or service is reasonable and necessary.
A detailed account of the methodological principles of study design that the Agency utilizes to assess the relevant literature on a therapeutic or diagnostic item or service for specific conditions can be found in Appendix A. In general, features of clinical studies that improve quality and decrease bias include the selection of a clinically relevant cohort, the consistent use of a single good reference standard, blinding of readers of the index test, and reference test results.
Public commenters sometimes cite the published clinical evidence and provide CMS with useful information. Public comments that provide information based on unpublished evidence, such as the results of individual practitioners or patients, are less rigorous and therefore less useful for making a coverage determination. Public comments that contain personal health information will be redacted or, in some cases, will not be made available to the public. CMS responds in detail to the public comments on a proposed national coverage determination when issuing the final decision memorandum.
VII. Evidence
A. Introduction
This section provides a summary of the evidence we considered during our review. The evidence reviewed to date includes the published medical literature on pertinent studies that link WCH and masked hypertension to end organ damage and death.
B. Discussion of Evidence
1. Evidence Question(s)
Our review and analysis of the evidence on the clinical utility of ABPM in patients with office-based elevated (white coat) blood pressure, and in patients being treated for hypertension who are suspected as having masked hypertension, is guided by the following questions:
- In patients with suspected white coat hypertension who are not on treatment for elevated blood pressure, does ABPM improve health outcomes?
- In patients with white coat hypertension, does ABPM improve health outcomes?
- In patients with suspected masked hypertension, does ABPM improve health outcomes?
2. External Technology Assessments
While CMS did not request an external technology assessment (TA) as part of this reconsideration, a structured literature review and meta-analysis that focused on the effects of blood pressure monitoring was conducted by the US Preventive Services Task Force (USPSTF) and published by the Agency for Healthcare Research and Quality (AHRQ) in 2014. It was published in condensed form in the Annals of Internal Medicine in 2015.
Piper MA, Evans CV, Burda BU, Margolis KL, O’Connor E, Smith N, Webber E, Perdue LA, Bigler KD, Whitlock EP. Screening for High Blood Pressure in Adults: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2014 Dec. Available from http://www.ncbi.nlm.nih.gov/books/NBK269495/ PMID: 25632496.
And
Piper MA, Evans CV, Burda BU, Margolis KL, O'Connor E, Whitlock EP. Diagnostic and predictive accuracy of blood pressure screening methods with consideration of rescreening intervals: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2015 Feb 3;162 (3):192-204. doi: 10.7326/M14-1539. PubMed PMID: 25531400.
The authors performed a technology assessment that included a systematic literature review and meta- analysis to support the USPSTF in updating its recommendation on screening for high blood pressure (BP) in nonpregnant individuals. The USPSTF report focused on screening for high BP. The USPSTF report evaluated the benefit of office based BP measurement and out-of-office measurement with an emphasis on ABPM.
The USPSTF assessment was based on key questions that examined evidence for the benefits and harms of screening for high BP, diagnostic accuracy of OBPM, prediction of cardiovascular events by BP method and diagnostic accuracy of non-office measurement, and rescreening interval. The authors searched MEDLINE, PubMed, the Cochrane Central Register of Controlled Trials, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) from 2003 through August 2014 to review the benefits and harms of screening for high BP. The review used studies that followed cohorts over time and reported the hazard or risk ratios of BP as a continuous variable, measured by at least 2 methods at baseline. The authors required all studies to be from highly developed countries and enrolled previously untreated adults. The authors reviewed 19,309 abstracts and 1171 articles.
To answer the question about the benefit of BP screening, the authors found one good quality cluster randomized controlled trial pharmacy-based BP screening of adults aged 65 years or older in Ontario Canada (Kaczorowski et al., 2011). This trial demonstrated fewer annual composite cardiovascular- related hospitalizations in the intervention group than in the control group (rate ratio 0.91 [95% CI, 0.86 to 0.97]; P = 0.002). When the data were analyzed by the number of unique patients hospitalized, only the reduction in admissions for acute myocardial infarction was statistically significant (rate ratio 0.89 [CI, 0.79 to 0.99]; P = 0.03). This study and its long term follow up are discussed in more detail later in this review.
In the authors’ evaluation of the diagnostic accuracy of office based BP measurement using manual sphygmomanometry as the reference standard, they found sensitivities ranging from 51% to 68% for elevated BP defined as systolic BP ≥140 mm Hg or diastolic BP ≥90 mm Hg in three studies. A fourth study reported a sensitivity of 91%, but differed from the others in that it used an elevated BP (systolic BP ≥160 mm Hg or diastolic BP ≥95 mm Hg) and a more stringent design to minimize human error. The specificities ranged from 92% to 97% (in the more stringent study) and positive predictive value (PPV; the probability that a particular patient has the disease, given a positive test result) ranged from 76% to 84%. They also evaluated the effect of repeated OBPM measurements, finding that in one large US study, 27.5% were reclassified using the mean of all three BP measurements for diagnosis, and 35.5% were reclassified as normal using the mean of the second and third BP measurements for diagnosis.
The authors conducted a meta-analysis to evaluate the best predictors of cardiovascular events by BP measurement method (ABPM, OBPM, and other out-of-office measurements). Where reported, all ABPM devices were oscillometric, and typically took measurements every 15 to 30 minutes during the day and every 30 to 60 minutes at night. Outcomes for 24-hour, daytime, and nighttime monitoring cycles were reported in 8, 10, and 9 studies, respectively. Results did not vary by geographic region or population baseline characteristics. Unadjusted hazard ratios (HRs) for systolic OPBM were not consistently statistically significant, ranging from 1.07 to 1.29 for stroke and 1.06 to 1.32 for CV events or mortality (Figure 1). This pattern of results for OBPM was similar across all ABPM versus OBPM comparisons and outcomes.
Figure 1 Risk for Cardiovascular and Mortality Outcomes: OBPM, Not Adjusted for 24-hour ABPM
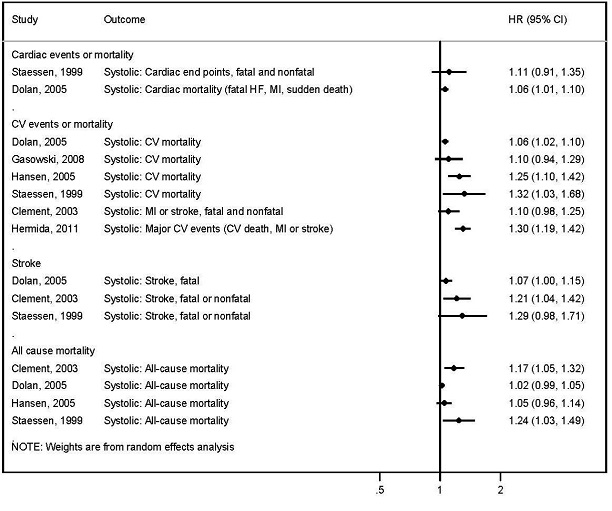
Abbreviations: CI = confidence interval; CV = cardiovascular; HF = heart failure; HR = hazard ratio; MI = myocardial infarction
Each 10-mm Hg increase in 24-hour systolic ABPM, adjusting for OPBM, was consistently associated with increased risk for fatal and nonfatal stroke events in four studies (Figure 2). Risk estimates ranged from an HR of 1.28 to 1.40 and were all statistically significant, indicating that systolic ABPM predicted stroke events statistically significantly and independently of OBPM. The largest risk estimate (HR 1.40 [95% CI, 1.21 to 1.62]) was reported for a community-based study in rural Japan, which enrolled 1,332 participants who were followed for a mean of 10.2 years. This study was the only study that did not limit participation to those with hypertension and had by far the lowest mean baseline OBPM (131/74 mm Hg). In 6 studies, each 10–mm Hg increment in 24-hour systolic ABPM, adjusted for OBPM, was associated with an increased risk for fatal and nonfatal cardiovascular events, which was statistically significant in 5 studies. Hazard ratios ranged from 1.11 to 1.42. The authors concluded that all studies reported lower event rates or risk estimates for participants with isolated clinic hypertension than for those with sustained hypertension.
Figure 2. Risk for Cardiovascular and Mortality Outcomes: Systolic 24-hour ABPM, Adjusted for OBPM
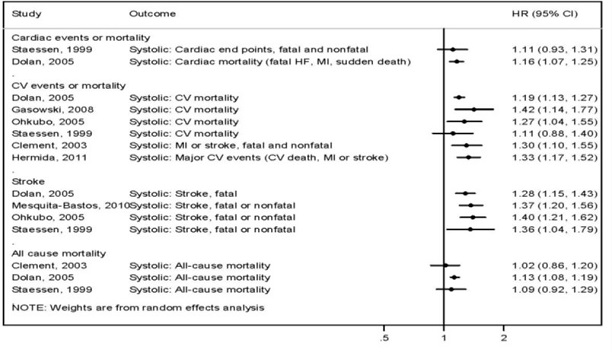
Abbreviations: CI = confidence interval; CV = cardiovascular; HF = heart failure; HR = Hazard ratio; MI = myocardial infarction.
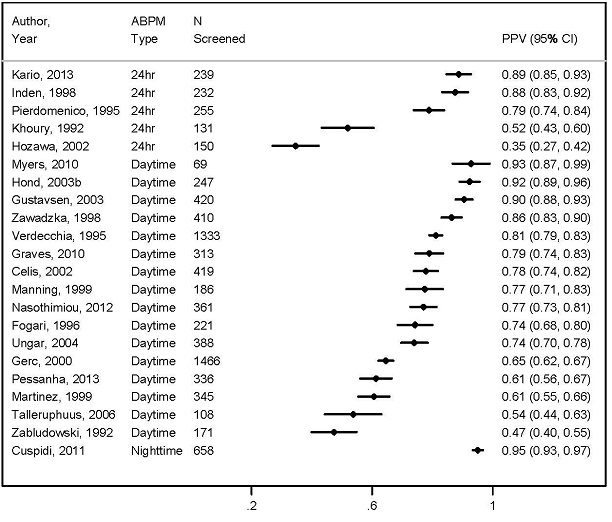
The authors evaluated the diagnostic accuracy of confirmatory BP measurement methods by using ABPM as the reference standard, subsequent to an elevated BP at screening. Daytime ABPM was measured in 18 nonoverlapping studies that evaluated diagnostic accuracy in 69 to 1,466 participants per study. The proportion of participants with elevated OBPM and true hypertension (as measured by daytime ABPM) ranged from 0.47 (95% CI, 0.40 to 0.55) to 0.93 (95% CI, 0.87 to 0.99) (Figure 3).
Figure 3. Proportion of Elevated Office-Based Screening Results that are Confirmed Hypertension by ABPM
The authors also evaluated whether there were any harms associated with BP screening and found no differences in psychological distress or quality of life when subjects were labeled as hypertensive or prehypertensive (excluding misdiagnosis and unnecessary treatment). There were, however, increases in overall absenteeism from work, absenteeism due to illness, and number and duration of illness episodes after labeling persons who were previously unaware of their hypertension status as hypertensive.
The authors concluded that ABPM (24-hour, daytime, or nighttime) is a better predictor of long-term CV outcomes than OBPM (manual sphygmomanometry) and should be considered the reference standard for evaluating BP noninvasively. Initial screening with office-based methods variably predicts hypertension, as defined by ABPM, resulting in a significant population with isolated clinic hypertension. Limited evidence suggested that people with isolated clinic hypertension have outcomes more like normotensive than hypertensive persons. Failure to confirm initial elevated OBPM results may result in misdiagnosis and overtreatment. Limited evidence suggested that repeated measurements and improved procedural control (e.g., automation) may improve the diagnostic accuracy of OBPM when used to screen for high BP or confirm hypertension in the office. Studies of rescreening intervals at up to 6 years found a higher incidence of hypertension overall and at shorter intervals for persons with BP in the high-normal range, older adults, persons with an above normal BMI, and African Americans. These studies showed much lower incidence at longer rescreening intervals (up to 6 years) in persons without these risk factors. Based on the results of their metaanalysis, the authors stated that failure to confirm initial elevated OBPM results may result in misdiagnosis and overtreatment.
3. Internal Technology Assessment
Literature Search Methods
We searched PubMed and the Cochrane Library from 2014, the year that the USPSTF assessment was published (Piper et al, 2014) to the present. Search terms included ambulatory blood pressure monitoring (ABPM), white coat hypertension (WCH), and masked hypertension. We looked for: 1) studies that evaluated the prevalence of WCH and masked hypertension in representative populations; 2) studies that evaluated the effect of WCH and masked hypertension or stroke, cardiovascular morbidity, and cardiovascular and all-cause mortality; and 3) studies on clinical utility of ABPM in predicting and improving health outcomes including cardiovascular outcomes and mortality compared to office based BP monitoring (OBPM). Our search terms included "blood pressure monitoring", "ambulatory blood pressure monitoring (both systolic and diastolic)", "cardiovascular diseases/morbidity/mortality", "all-cause mortality", "stroke" , "white coat hypertension", "uncontrolled hypertension", "office blood pressure", "isolated clinic hypertension", and "masked hypertension". We excluded studies of home blood pressure monitoring. We identified two meta- analyses, one randomized control trial, six analyses of population based prospective longitudinal cohorts, and one nested case-control study. We also reviewed references submitted to us by the requester and commenters and performed a hand search of bibliographies to identify other pertinent articles.
Kaczorowski J, Chambers LW, Dolovich L, et al. Improving cardiovascular health at population level: 39 community cluster randomised trial of Cardiovascular Health Awareness Program (CHAP). BMJ. 2011 Feb 7;342:d442.
The aim of this study was to evaluate the effectiveness of the community based Cardiovascular Health Awareness Program (CHAP) on morbidity from cardiovascular disease. This was a randomized trial of municipalities (n=41) in Ontario Canada with populations of 10 to 60 thousand. The study was based in 39 of these municipalities (2 of the 41 were the location of the pilot test) with a total population of 973,246, including 140,542 people older than age 65 years. The 39 communities were stratified by population size and geographical location. The intervention (CHAP [n=20] vs. no intervention [n=19]) was randomly allocated to each stratum. Availability of usual health promotions and services was unchanged.
The CHAP intervention was delivered by peer volunteers and consisted of 10 weeks of 3-hour weekday blood pressure and cardiovascular risk factor assessment and educational sessions held concurrently in all 20 intervention communities during the autumn of 2006. Blood pressure readings and other information on cardiovascular risk factors were recorded, provided to each participant, and with participants’ consent sent to their family physician and usual pharmacist. Of interest to this review is the out-of-office blood pressure program. Evaluation of the program relied on routinely collected population based administrative health data, including hospital discharge abstracts from the Canadian Institute for Health Information, physician service claims from the Ontario Health Insurance Program, and prescription drug claims from the Ontario Drug Benefit Program.
The primary outcome measure was the change in the mean annual rate of hospital admissions with a "most responsible" (primary) discharge diagnosis of acute myocardial infarction, congestive heart failure, or stroke (composite end point) among community dwelling residents aged 65 years and over in the year before compared with the year after implementation of CHAP. Secondary outcome measures were mortality during the above hospital admissions, all-cause mortality, and newly prescribed antihypertensive drug treatment. Hospital admissions of interest occurred between September 1, 2005 and August 31, 2006 ("pre-intervention period") and between September 1, 2007 and August 31, 2008 ("post-intervention period"). The denominator was the number of community dwelling people aged 65 years and over who were alive and residing in each study community on the first day of the pre-intervention period.
The mean number of residents aged 65 years and over in the 39 study communities was 3606, their mean age was 74.8 years, and 42.8% were male. There were statistically significant differences between the control and intervention communities with respect to rurality (28.96% vs. 31.63% rural), income status (16.95% vs. 18.57% lowest income quantile), average number of prescription drugs in the previous year (7.25 vs. 6.98), Charlson comorbidity index (0.57 vs. 0.58), history of heart failure (12.19% vs. 12.45%), and death rate per 1000 (3.45 vs. 3.55).
The authors found statistically significant reductions favoring the intervention communities in hospital admissions for acute myocardial infarction (RR 0.87, 95% CI 0.79 to 0.97) and congestive heart failure (RR 0.90, 95% CI 0.81 to 0.99) but not for stroke (RR 0.99, 95% CI 0.88 to 1.12) for community residents aged 65 years and older (Table 3). These numbers may have included multiple admissions per person. A second analysis of individuals aged 65 and older, found statistically significant difference favoring the CHAP intervention in newly prescribed antihypertensive drug treatment (RR 1.10, 95% CI 1.02 to 1.20), a trend towards lower in hospital cardiovascular mortality (RR 0.86, 95% CI 0.73 to 1.01), and no difference in all-cause mortality (RR 0.98, 95% CI 0.92 to 1.03).
| Table 3 Comparison of mean hospital admission rates per 1000 by study arm |
|---|
|
Pre-intervention rate |
Post-inervention rate |
Hospital
admissions |
CHAP
(n=67 874) |
Control
(n=72 768) |
CHAP
(n=69 942) |
Control
(n=75 499) |
Rate ratio
(95% CI) |
| Composite |
30.15 |
29.36 |
27.90 |
30.13 |
0.91 (0.86 to 0.97) |
| Acute myocardial infarction |
10.24 |
10.26 |
9.54 |
10.81 |
0.87 (0.79 o 0.97) |
| Congestive heart failure |
11.19 |
11.11 |
10.51 |
12.22 |
0.90 (0.81 to 0.99) |
| Stroke |
8.71 |
7.99 |
7.86 |
7.10 |
0.99 (0.88 to 1.12) |
The authors discussed the following limitations: 1) the specific components of CHAP that were responsible for the observed reductions in hospital admissions are unknown; 2) other environment factors may have been at play such as an increase in the rate of newly prescribed antihypertensive treatment or improved adherence to guidelines for starting of drug treatment or lifestyle changes in the CHAP communities.
The authors concluded that the CHAP community based health promotion and prevention program targeted at older adults can reduce cardiovascular morbidity at the population level.
Dahrouge S, Kaczorowski J, Dolovich L, et al. Long term outcomes of cluster randomized trial to improve cardiovascular health at population level: The Cardiovascular Health Awareness Program (CHAP). PLoS One. 2018 Sep 6;13(9):e0201802.
This study evaluated the impact of the CHAP intervention on morbidity and mortality related to cardiovascular events over the five years after the intervention. The authors followed all community- dwelling individuals 65 years of age and older who were eligible for the CHAP cluster randomized as described above from September 1, 2006 through August 31, 2011 using administrative health data. All residents of the 39 communities meeting the study eligibility criteria as of the intervention start date were identified to form the study cohort. The list was limited to individuals 65 years of age or older using a registered persons database, and to those residing in the community, and excluding residents of long term care facilities identified from a continuing care reporting system. The dataset comprised 143,976 individuals, 69,318 and 74,658 in the intervention and control communities, respectively, which was followed for 5 years.
The main outcome was CVD-related hospitalizations; a composite endpoint indicating hospitalizations for which the most responsible diagnosis was stroke, CHF, or acute myocardial infarction. Secondary outcomes included hospitalizations for each condition separately, CVD-related in-hospital deaths and all-cause mortality. All analyses were intention-to-treat. The primary analytic endpoint was the count of CVD-related hospitalizations (Event level) per cumulative 100 person- years follow-up. Secondary outcomes included the rate of hospitalizations for each reason separately, mortality rates, and rates of individuals having at least one hospitalization (individual level). They used Kaplan-Meier plots to visually depict the time to first event for each outcome and assessed the hazard of an individual having the outcome of interest over time using a Cox regression model with frailty (random effects) to account for clustering at the community level and adjusting for the pre-intervention baseline rate of the outcome.
The five-year cumulative rate ratio [95% confidence interval (CI)] for CVD-related hospitalizations was 0.958 [0.898±1.022], translates into an estimated 408 averted hospitalizations, or 5.9 per 1,000 individuals over the five-year period. Most estimates pointed to an advantage for individuals residing in the intervention communities, but only the hazard ratio for all-cause mortality was significantly different across the groups (HR [CI] = 0.955 [0.914±0.999], p = 0.0429). Accounting for the ruralit status of the individuals in the community in the post hoc analyses, the rate ratio [CI] 0.855 [0.750±0.976]) and HR 0.862 [0.770±0.965] of death occurring during CVD-related hospitalizations were statistically significantly in favor of the intervention arm.
The authors acknowledged the following limitations: 1) Because the study relied exclusively on health administration data, there was not access to information that could help elucidate the findings such as determining participants' access to the recommended resources, and assessing changes in patient health behaviors, blood pressure levels, or other factors that could have helped explain the pathway through which the intervention imparted cardiovascular protection; 2) There was no data on the intensity with which the intervention communities maintained CHAP activities and how these might have been adapted to help understand the impact of these factors on the intervention 5-year effectiveness measures; 3) There were too few communities to allow an assessment of community resources available to participants; 4) The closed cohort approach did not account for migration of individuals across communities; 5) The increased awareness of cardiovascular disease could have led to an increased likelihood of assigning cardiovascular disease as a reason for hospitalization; and 6) The small number of clusters in the study may have reduced the study power. The last three limitations would reduce the ability of the study to find differences.
The authors concluded that there was a consistent pattern favoring better health outcomes in the intervention compared to the control communities, with all-cause mortality reaching statistical significance. They concluded that the results suggest an apparent reduction in morbidity and mortality in the intervention arm over the five-year period with no evident attenuation of the observed effect over time, demonstrating a 9% reduction in the risk of CVD hospitalization in the first year following the intervention year and an average 4% [-2%-10%] risk reduction in the five years following the intervention: a lower yearly estimate, but potentially prolonged clinically meaningful consequences.
Banegas JR, de la Cruz JJ, Graciani A, et al. Impact of Ambulatory Blood Pressure Monitoring on Reclassification of Hypertension Prevalence and Control in Older People in Spain. J Clin Hypertens (Greenwich). 2015 Jun;17(6):453-61.
The aim of this study was to estimate the impact of ABPM on the prevalence and control of BP in older adults in Spain, to allow quantification of overtreatment or undertreatment and obtain a balanced view of the burden of hypertension in the population. This was an observational, cross- sectional analysis using data collected in the second wave (2012) of the Spanish Nutrition and Cardiovascular Risk Survey (ENRICA). Participants were randomly selected from the Spanish population aged 60 years and older. The second wave consisted of 2519 individuals and included a phone interview on health status, lifestyle, and morbidity; and a home visit to record BP, body mass measurements, diet, and medication. ABPM was offered to 1698 individuals and performed in 1328 patients (response rate, 78.2%). Casual BP was measured with validated automatic devices three times at 2-minute intervals after the patients rested for 5 minutes in a seated position and calculated as the mean of the last two readings. ABPM was performed with a validated oscillometric device programmed to read BP at 20-minute intervals during the day and at 30-minute intervals during the night for 24-hours.
There were 1047 patients with 70% or more valid ABPM readings. The authors grouped patients by casual BP into 2 hypertension categories: 720 hypertensive (casual BP threshold ≥140/90 mm Hg) and 327 normotensive patients. They also grouped the patients by treatment status, antihypertensive drug treated (n=514) and untreated (n=533) patients. The latter included 206 untreated hypertensives and 327 normotensives. They used these categories to calculate the percentage of hypertensive patients according to casual BP and according to ABPM; and the percentage of patients at BP goal according to casual BP and according to ABPM. The authors then calculated the percentage of patients reclassified from above casual BP goal to the ABPM goal, and those reclassified the casual BP goal to above ABPM goal for the total sample and by BP medication status.
The mean age of patients was 71.7 years, 50.8% were men, mean BMI was 28.1 kg/m2, 14.9% had diabetes, and 5.7% had previous CVD. Mean casual BP was 137.8/74.0 mm Hg, mean 24-hour BP was 123.6/69.8 mm Hg. Hypertensive patients were older, more likely to be obese and have diabetes than normotensive patients. Treated hypertensive patients were older, with higher BMI and higher frequency of obesity, diabetes, and history of CVD than untreated patients. Mean casual and ambulatory SBPs were higher in treated hypertensive patients than untreated participants. There was only moderate correlation between casual BP and ABPM.
Compared with participants without ABPM, those with a 24-hour ABPM had similar age (71.8 years vs. 71.7 years), proportion of men (47% vs. 49%), education level (63% vs. 61% with ≤ primary studies), mean body mass index (BMI; 27.8 vs. 27.5 kg/m2), proportion of diabetes (15.1% vs. 16.1 %), current smoking (11.0% vs. 11.7%), and history of cardiovascular disease (CVD; 5.7% vs. 4.5%).
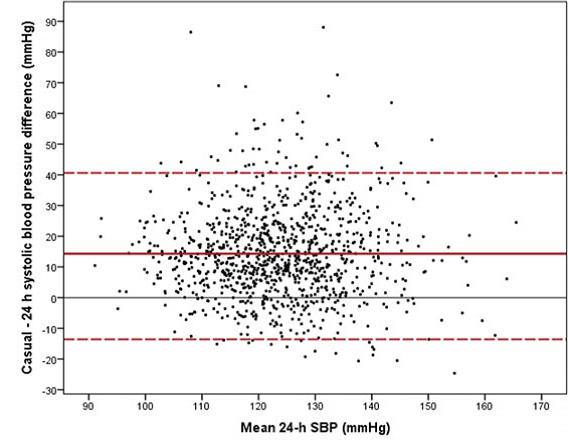
The scatterplot (Figure 3) shows a marked overestimation of casual SBP compared to ambulatory SBP. The mean difference between casual and 24-hour SBP was 14.3 mm Hg.
Figure 4. Bland-Altman plot for the association between casual and ambulatory s (SBP)

There were 596 patients within casual BP normotensive range (56.9% CI, 53.9%–59.9%) and 749 were at 24-hour BP normal range or goal (71.5%; 95% CI 68.8%–74.2%; absolute difference, 14.6%; P<.001) (Table 4). There were 269 treated hypertensive patients at casual BP goal (52.4%) and 352 at 24-hour BP goal (68.5% difference, 16.1%; P<.001). There were 720 casual BP–based hypertensive patients and 650 ABPM–based hypertensive patients eligible for treatment. BP control among these patients with treatment-eligible hypertension increased from 37.4% with a casual BP target to 54.1% with a 24-hour ABPM target (absolute difference, 16.7%; P<.01). Total reclassifications were 21.7% from above normal casual BP to a normal 24-hour BP, and 7.1% from a normal casual BP to above normal 24-hour BP.
| TABLE 4. Reclassification of BP Control Status According to Ambulatory Monitoring by Treatment Status. |
|---|
| Casual BP |
At casual and 24-hour BP Goal |
Reclassified to Above 24-hour BP Goal |
Not Hypertensive or at Casual BP |
<140/90 mmHg |
|
|
|
Total |
522 (49.9%) |
74 (7.1%) |
596 (56.9%) |
| Untreated |
294 (55.2%) |
33 (6.2%) |
327 (61.4%) |
| Treated |
228 (44.4) |
41 (8.0%) |
269 (52.3%) |
|
Reclassified to 24-hour BP Goal |
Above Casual and 24-hr BP Goal |
Above Casual BP Goal |
| ≥140/90 mmHg |
|
|
|
| Total |
227 (21.7%) |
224 (21.4%) |
451 (43.1%) |
| Untreated |
103 (19.3%) |
103 (19.3%) |
206 (38.6%)
|
| Treated |
124 (24.1%) |
121 (23.5%) |
245 (47.7%) |
| Abbreviations: BP, blood pressure; treated, hypertensive patients taking current BP medication; untreated, normotensive and untreated hypertensive patients. |
The authors acknowledged the following limitations: 1) The study was not representative of the general older population of Spain preventing population extrapolations; 2) Casual BP was not measured in the office but in patients’ homes, likely diminishing a reaction alarm and giving more realistic BP estimates; and 3) The issue of selecting BP threshold was not, at the time, settled, but the direction of the results was consistent; casual BP overestimates the true (ambulatory) hypertension prevalence and greatly underestimates the BP control among treatment-eligible patients; therefore, upward and downward BP reclassification is noticeable, suggesting a potential benefit of ABPM as compared with casual BP.
The authors concluded that compared with casual BP, 24-hour ABPM led to a reduction in the proportion of patients recommended for hypertension treatment and a substantial increase in the proportion of those with hypertension control.
Banegas JR, Ruilope LM, de la Sierra A, et al. Clinic Versus Daytime Ambulatory Blood Pressure Difference in Hypertensive Patients: The Impact of Age and Clinic Blood Pressure. Hypertension. 2017 Feb;69(2):211-219.
The aim of this study was to compare OBPM and ABPM values across a wide age spectrum in a population based adult cohort from the Spanish ABPM Registry. The authors identified 115,708 individuals in the Registry who had complete information on clinical characteristics and good quality ABPM data. A total of 104,639 of these were hypertensive based an OBPM ≥140/90, forming the analytic cohort.
OBPM was the average of 2 office-based BP readings after the patient had been resting in a seated position for 5 minutes. ABPM was performed with automated oscillometric devices. Variables used in the analysis were based on interviews and physical examination at the time of the initial visit and on data from clinical records. The variables included age, sex, obesity (BMI ≥30 kg/m2), cardiovascular risk factors including smoking (active use in the last year), dyslipidemia (total cholesterol >4.9 mmol/L, low-density lipoprotein cholesterol >3 mmol/L, or high-density lipoprotein cholesterol <1.0 mmol/L in men or <1.2 mmol/L in women, or fasting triglycerides >1.7 mmol/L or use of lipid-lowering drugs), diabetes (plasma fasting glucose ≥7 mmol/L or use of antidiabetic drugs), and previous coronary or cerebrovascular event, heart failure hospitalization, coronary or peripheral revascularization documented in the clinical record.
Mean age of the cohort was 59.3 years, 53.4% were men, mean OBPM was 150.6/87.8 mm Hg, mean daytime ABPM was 133.2/79.5 mm Hg, mean BMI was 29.9 kg/m2, 67.8% of patients had treated hypertension, and the mean number of BP medications among treated patients was 2.1. Mean age of treated hypertensives was 61.8 years and that of untreated hypertensives was 54.0 years. In the whole cohort and in the treated and untreated hypertensive groups, mean OBPM SBP and DBP were generally significantly higher than their mean daytime ABPM counterparts within each 10 year age group (P<0.05).
The frequency of WCH was 36.7%, and 52.7% in those at SBP of 140 to 149 mm Hg (49.5% within SBP 140–159 mm Hg), and generally increased with age and decreased with OBPM. The frequency of masked hypertension was 3.9%, amounting to 23% in those treated with a clinic SBP of 130 to 139 mm Hg, and generally decreased with age and increased with office based SBP. Misclassification of hypertension status by OBPM alone was over 40%.
Table 5. Prevalence of White-Coat Hypertension and Masked Hypertension, by Age and Treatment Status in a Spanish Population of Hypertensive Patients
| Age, y |
N |
White-Coat Hypertension, % |
Masked Hypertension, % |
| Treated hypertensive patients |
| Total |
70,997 |
34.6 (34.3/35.0) |
5.8 (5.6/6.0) |
| 18–29 |
671 |
30.3 (26.8/33.8) |
7.5 (5.5/9.5) |
| 30–39 |
2,752 |
29.1 (27.4/30.8) |
8.9 (7.8/10.0) |
| 40–49 |
9,165 |
28.7 (27.8/29.6) |
8.2 (7.6/8.8) |
| 50–59 |
16,762 |
32.6 (31.9/33.3) |
6.2 (5.8/6.6) |
| 60–69 |
19,911 |
37.4 (36.7/38.1) |
5.2 (4.9/5.5) |
| 70–79 |
16,670 |
37.8 (37.1/38.5) |
4.5 (4.2/4.8) |
| 80–89 |
4,853 |
34.2 (32.9/35.5) |
4.9 (4.3/5.5) |
| ≥90 |
213 |
33.8 (27.4/40.2) |
4.9 (2.0/7.8) |
| P Value |
… |
<0.001 |
<0.001 |
| Untreated hypertensive patients |
| Total |
33,642 |
41.3 (40.8/41.8) |
… |
| 18–29 |
1,702 |
50.5 (48.1/52.9) |
… |
| 30–39 |
3,416 |
39.4 (37.7/41.0) |
… |
| 40–49 |
7,350 |
34.2 (33.1/35.3) |
… |
| 50–59 |
9,150 |
38.3 (37.3/39.2) |
… |
| 60–69 |
7,179 |
46.3 (45.1/47.5) |
… |
| 70–79 |
3,934 |
48.9 (47.3/50.5) |
… |
| 80–89 |
874 |
46.3 (43.0/49.6) |
… |
| ≥90 |
37 |
35.1 (19.7/50.5) |
… |
| P Value |
… |
<0.001 |
… |
| Results are presented as percentages (95% confidence interval). White-coat hypertension: OBPM SBP ≥140 or DBP ≥90 mm Hg and daytime ABPM
SBP/DBP <135/<85 mm Hg. Masked hypertension: OBPM SBP/DBP <140/<90 mm Hg and daytime ABPM SBP ≥135 or DBP ≥85 mm Hg. |
The overall difference between OBPM and ABPM was 17.4 mm Hg. The unadjusted magnitude of the OBPM minus mean daytime ABPM increased significantly and consistently from age 30 to age 80 years (P<0.001). Age, cardiovascular risk variables, and OBPM were significantly associated with all the OBPM-mean daytime ABPM differences in a multivariable analysis.
The range of variation in BP differences among age decades for each OBPM decile was much narrower than the range of variation in BP differences along the OBPM continuum, indicating a greater influence of OBPM that age on BP differences. In general, among treated and untreated hypertensive patients, OBPM values tended to be higher than daytime ABPM values. This was true for >95% of subjects and above a clinic BP value of ≈120/75 mm Hg
The authors acknowledged the following limitation: although the study was performed on a large single cohort of more than 100 000 hypertensive people and the Spanish ABPM registry provides a real-world view of clinical practice, any registry study has inherent potential sources of bias. Two seated BP readings from a single visit were averaged to characterize clinical BP, and the mean clinic–ambulatory BP difference.
The authors concluded that in this cohort of hypertensive patients seen in usual clinical practice, mean daytime ABPM was generally lower than OBPM at all ages, and OBPM minus mean daytime ABPM are largely a function of the OBPM. These findings were consistent throughout hypertension treatment status, reproducible in the medium term, and robust to different ambulatory BP criteria (daytime, 24-hour, or nighttime) in a sensitivity analysis. Of practical importance, white-coat hypertension (i.e., ABPM is normal) is unlikely to occur once the clinic BP is grade 2 or above and is most likely to occur in those with grade 1 hypertension. Thus, for the diagnosis of hypertension, if the availability of ABPM is restricted, then it would be best deployed to rule out white coat hypertension in patients with grade 1 hypertension according to clinic BP. Conversely, masked hypertension is more likely to occur in patients with borderline hypertension according to clinic BP. The authors also suggest that reliance on BP alone taken during an office visit is often inadequate to assess and optimize BP control because many patients have a significant white-coat or masked hypertension, leading to underestimation or overestimation of BP control, respectively. They acknowledge that further studies are needed to assess the impact of using ABPM more widely on clinical outcomes and define the cost-effectiveness of such an approach.
Banegas JR, Ruilope LM, de la Sierra A, et al. Relationship between Clinic and Ambulatory Blood- Pressure Measurements and Mortality. N Engl J Med. 2018 Apr 19;378(16):1509-1520.
The aim of this study was to evaluate the prognostic value of clinic and ambulatory blood pressures as well as of hypertension phenotypes such as white coat hypertension and masked hypertension, on total and cardiovascular mortality.
This was an observational study of a cohort of patients from the Spanish Ambulatory Blood Pressure Registry, a national study of patients 18 years of age or older selected by their physicians at 223 primary care centers who were enrolled in the registry between March 1, 2004, and December 31, 2014. Patients were required to meet European guideline-recommended indications for ambulatory blood-pressure monitoring. Blood pressure was the average of 2 office-based BP readings after the patient had been resting in a seated position for 5 minutes. ABPM was performed with automated oscillometric devices. The date and cause of death came from a search of the vital registry of the Spanish National Institute of Statistics.
Hypertension phenotypes in untreated patients were defined as:
- White-coat hypertension: clinic SBP≥140 mm Hg or DBP≥90 mm Hg and 24-hour SBP<130 mm Hg and DBP <80 mm Hg.
- Uncontrolled or masked hypertension: clinic SBP <140 mm Hg and DBP <90 mm Hg and 24- hour SBP ≥130 mm Hg or DBP ≥80 mm Hg.
- Sustained, uncontrolled hypertension: clinic SBP ≥140 mm Hg or DBP ≥90 mm Hg and ambulatory 24-hour SBP ≥130 mm Hg or DBP ≥80 mm Hg.
- Normotension: clinic SBP <140 mm Hg and DBP <90 mm Hg and 24-hour SBP <130 mm Hg and DBP <80 mm Hg.
The authors developed survival models adjusting for age, sex, smoking, body mass index, diabetes, dyslipidemia, previous cardiovascular disease, and number of antihypertensive drugs used; and in a second model, clinic blood pressure was adjusted for 24-hour blood pressure; 24-hour pressure was adjusted for clinic pressure; daytime pressure was adjusted for clinic and nighttime pressure; nighttime pressure was adjusted for clinic and daytime pressure. Hazard ratios (HRs) were calculated per 1-SD increment in BP pressure, and for hypertension phenotypes the reference group was normotension. The authors calculated rate advancement periods to estimate the number of additional years of chronologic age that would be required to yield the equivalent mortality rate per 1-SD increase in blood pressure or for each hypertension phenotype compared with normotension; and population attributable fractions to estimate the fraction of mortality in the population that could be attributed to each hypertension phenotype.
There were 64,910 patients in the study. The mean age of the study participants was 58.4±14.2 years, 58% were men, the mean clinic blood pressure was 147.9/86.7 mm Hg, and the mean 24-hour ambulatory blood pressure was 129.2/76.5 mm Hg. The median follow-up was 4.7 years. There were 3808 (6%) deaths during the study period; 1295 (34%) of these were from cardiovascular disease.
The results of the Cox proportional hazards model are reproduced in Table 6. In the model (Model 2) that included both 24-hour and clinic measurements, 24-hour SBP was more strongly associated with all-cause mortality (hazard ratio 1.58 per 1-SD increase in pressure; 95% confidence interval [CI], 1.56 to 1.60, after adjustment for clinic BP) than the clinic SBP pressure (hazard ratio 1.02; 95% CI, 1.00 to 1.04, after adjustment for 24-hour blood pressure). The associations were nearly identical for cardiovascular mortality.
| Table 6 Association of Clinic and Ambulatory Blood Pressure with All-Cause and Cardiovascular Mortality in 2 Cox Regression Models |
|---|
| |
Model 1 |
Model 2 |
| All-cause mortality |
Hazard Ratio (95% CI) |
Hazard Ratio (95% CI) |
| |
Clinic SBP |
1.54 (1.52–1.56) |
1.02 (1.00–1.04) |
| |
Clinic DBS |
1.02 (1.00–1.04) |
0.89 (0.87–0.92) |
| |
24-hour SBP |
1.58 (1.56–1.60) |
1.58 (1.56–1.60) |
| |
24-hour DBP |
1.56 (1.54–1.58) |
1.56 (1.54–1.59) |
| |
Daytime SBP |
1.57 (1.55–1.60) |
1.54 (1.52–1.56) |
| |
Daytime DBS |
1.55 (1.53–1.58) |
1.01 (0.99–1.04) |
| |
Nighttime SBP |
1.57 (1.55–1.59) |
1.55 (1.53–1.57) |
| |
Nighttime DBS |
1.56 (1.54–1.59) |
1.56 (1.54–1.59) |
| Cardiovascular mortality |
|
|
| |
Clinic SBP |
1.54 (1.52–1.56) |
1.02 (1.00–1.04) |
| |
Clinic DBS |
1.02 (0.99–1.04) |
0.89 (0.86–1.00) |
| |
24-hour SBP |
1.58 (1.55–1.60) |
1.58 (1.55–1.60) |
| |
24-hour DBP |
1.55 (1.53–1.58) |
1.56 (1.53–1.59) |
| |
Daytime SBP |
1.57 (1.55–1.60) |
1.54 (1.52–1.57) |
| |
Daytime DBS |
1.55 (1.52–1.58) |
1.01 (0.98–1.04) |
| |
Nighttime SBP |
1.57 (1.54–1.59) |
1.55 (1.53–1.57) |
| |
Nighttime DBS |
1.56 (1.53–1.59) |
1.56 (1.53–1.59) |
|
Model 1 was adjusted for age, sex, smoking status, body mass index, and status with respect to diabetes, dyslipidemia, previous cardiovascular disease, and number of antihypertensive drugs used.
Model 2 was additionally adjusted for clinic systolic and diastolic blood pressures.
Hypertension phenotypes were defined as follows in untreated patients: normotension= systolic <140 mm hg and diastolic <90 mm hg and normal 24-hour pressure (systolic <130 mm hg and diastolic <80 mm hg); white-coat hypertension = systolic ≥140 mm hg or diastolic ≥90 mm hg and normal 24-hour pressure; masked hypertension= normal clinic blood pressure and elevated 24-hour pressure (systolic ≥130 mm hg or diastolic ≥80 mm hg); and sustained hypertension= elevated clinic and 24-hour blood pressures. In treated patients, the corresponding terms were controlled hypertension, white-coat uncontrolled hypertension, masked uncontrolled hypertension, and sustained uncontrolled hypertension, respectively, and were defined with the same blood-pressure cutoff points as those used for untreated patients. |
Of all the hypertension phenotypes evaluated, masked hypertension was associated with the highest risk and showed a stronger association with all-cause mortality (hazard ratio, 2.83) than sustained hypertension (hazard ratio, 1.80) or white coat hypertension (hazard ratio, 1.79) when adjusted for clinic blood pressure (Table 7). Results for treated patients were similar to those for untreated patients, except that the results for white coat uncontrolled hypertension did not reach statistical significance (model 2 in Table7).
| Table 7 Association of Hypertension Phenotypes with All-Cause and Cardiovascular Mortality in 2 Cox Regression Models |
|---|
Mortality and Blood-Pressure Phenotype |
Model 1 |
Model 2 |
| |
All-cause mortality |
All Patients |
Deaths |
Hazard Ratio (95% CI) |
Hazard Ratio (95% CI) |
| |
Normotension |
4,221 |
76 |
Reference |
Reference |
| |
Controlled hypertension |
6,692 |
202 |
0.76 (0.57–0.99) |
0.81 (0.62–1.07) |
| |
White-coat hypertension |
6,628 |
309 |
2.24 (1.74–2.88) |
1.79 (1.38–2.32) |
| |
White-coat uncontrolled hypertension |
11,042 |
669 |
1.30 (1.01–1.66) |
1.06 (0.82–1.37) |
| |
Masked hypertension |
2,278 |
113 |
2.92 (2.18–3.90) |
2.83 (2.12–3.79) |
| |
Masked uncontrolled hypertension |
3,092 |
237 |
1.89 (1.44–2.47) |
1.96 (1.50–2.56) |
| |
Sustained hypertension |
12,555 |
595 |
2.36 (1.86–2.99) |
1.80 (1.41–2.31) |
| |
Sustained uncontrolled hypertension |
17,402 |
1607 |
1.90 (1.49–2.42) |
1.43 (1.11–1.85) |
|
Cardiovascular mortality |
|
Normotension |
4,221 |
22 |
Reference |
Reference |
|
Controlled hypertension |
6,692 |
84 |
0.90 (0.55–1.46) |
0.95 (0.59–1.55) |
|
White-coat hypertension |
6,628 |
94 |
2.36 (1.49–3.76) |
1.96 (1.22–3.15) |
|
White-coat uncontrolled hypertension |
11,042 |
223 |
1.23 (0.78–1.94) |
1.04 (0.65–1.66) |
|
Masked hypertension |
2,278 |
32 |
2.92 (1.70–5.03) |
2.85 (1.66–4.90) |
|
Masked uncontrolled hypertension |
3,092 |
95 |
2.20 (1.36–3.55) |
2.27 (1.41–3.68) |
|
Sustained hypertension |
12,555 |
172 |
2.42 (1.55–3.78) |
1.94 (1.23–3.07) |
|
Sustained uncontrolled hypertension |
17,402 |
573 |
1.93 (1.23–3.01) |
1.57 (1.00–2.47) |
| Model 1 was adjusted for age, sex, smoking status, body mass index, and status with respect to diabetes, dyslipidemia, previous cardiovascular disease, and number of antihypertensive drugs used.
Model 2 was additionally adjusted for clinic systolic and diastolic blood pressures.
Hypertension phenotypes were defined as follows in untreated patients: normotension= systolic <140 mm hg and diastolic <90 mm hg and normal 24-hour pressure (systolic <130 mm hg and diastolic <80 mm hg); white-coat hypertension = systolic ≥140 mm hg or diastolic ≥90 mm hg and normal 24-hour pressure; masked hypertension= normal clinic blood pressure and elevated 24-hour pressure (systolic ≥130 mm hg or diastolic ≥80 mm hg); and sustained hypertension= elevated clinic and 24-hour blood pressures. In treated patients, the corresponding terms were controlled hypertension, white-coat uncontrolled hypertension, masked uncontrolled hypertension, and sustained uncontrolled hypertension, respectively, and were defined with the same blood-pressure cutoff points as those used for untreated patients. |
The authors calculated rate advancement periods to estimate the number of additional years of age that would be required to yield the equivalent mortality rate per 1-SD increase in BP pressure or for each hypertension phenotype as compared with normotension. The rate advancement period for all-cause mortality was 1.4 years per 1-SD increase in clinic systolic blood pressure compared to 9.4 years per 1-SD for WCH and 22.6 years or masked hypertension per 1-SD increase in ambulatory systolic blood pressure.
The authors acknowledged the following limitations: 1) Clinic blood pressure represented the average of only two readings at each clinic visit; thus, the mean clinic pressure could be overestimated because it tends to become lower with repeated measurements; 2) In most patients, ambulatory blood- pressure monitoring was performed at a single time point, limiting its prognostic power; 3) There was data on medication during the follow-up period except in patients who had two ambulatory blood- pressure monitoring sessions; in these patients, the main study associations did not vary according to the number of medications received; 4) There may have been selection bias from inclusion criteria for ambulatory BP monitoring; 5) This was an observational study, thus, no direct inference can be made regarding the benefit of basing treatment on ambulatory blood-pressure measurements; and 6) The population studied was white and the results may not apply to people of other races.
The authors concluded that 24-hour, daytime and nighttime ambulatory systolic blood pressures were all better predictors of all-cause and cardiovascular mortality than clinic blood pressure. They also concluded that sustained hypertension, white coat hypertension, and masked hypertension were all associated with an increased risk of death; the strongest association was found with masked hypertension.
Franklin SS, Thijs L, Asayama K, et al. IDACO Investigators. The Cardiovascular Risk of White-Coat Hypertension. J Am Coll Cardiol. 2016 Nov 8;68(19):2033-2043.
The aim of this study was to address the possible increased CVD risk in persons with WCH in a community-based population. The observational data came from the International Database on Ambulatory Blood Pressure Monitoring in Relation to Cardiovascular Outcomes (IDACO) made up of people residing in the community from 12 randomly recruited cohorts with validated information on outcome, with standard protocols for conventional BP measurement and ABPM, most of whom were not treated with antihypertensive drugs.
This was a nested case-control study. In an initial sample of 12,148 participants (one cohort was excluded because of the imbalanced BP distribution compared to the 11 other cohorts), the authors excluded people <18 years, those with unavailable BP, those taking antihypertensive drugs at baseline, those with <10 daytime ambulatory BP readings, and those with missing information on 1 or more risk factors, leaving a total of 8,582 subjects of whom 5,137 were normotensive and 653 had WCH. In a matched case cohort design, the 653 patients with WCH were matched with 653 ormotensive controls, by cohort and age within 5 years and a risk score comprised of male sex; current smoking; dyslipidemia, defined as total cholesterol >4.9 mmol/l; and obesity, defined as body mass index >30 kg/m2. The risk score was 1= no risk factor; 2=1 to 2 risk factors; 3=≥3 risk factors; 4=diabetes without risk factors; and 5=history of CVD events or diabetes with other risk factors. Subjects were classified into low-risk (risk categories 1 and 2) or high-risk (risk categories 3, 4, and 5) groups. The authors used Kaplan-Meier survival function estimates and the Cox proportional hazards model to compare the incidence of CVD morbidity and mortality between WCH participants and their matched normotensive comparators. The authors defined WCH as conventional hypertension in the presence of a normal daytime ABPM and the white coat effect (WCE) as the systolic or diastolic conventional BP minus the daytime ABPM.
The prevalence of WCH among subjects with a normal daytime ABPM was 11.3% before matching. Compared with the normotensive group, subjects with WCH were older by 11.9 years, had a 14.7% greater male prevalence, had a significant increase in CVD risk factors, and had a higher prevalence of diabetes and prior CVD events. After matching, there were 494 patients each in the normotension and WCH in the low risk group, and 159 patients each in the normotension and WCH in the high risk group. Body mass index and the 24-hour systolic BP values were significantly higher (p < 0.05) in the WCH subjects as compared with the normotensive control subjects in both the low- and high-risk groups.
The 653 subjects with WCH and their normotensive control subjects were followed for a median of 10.8 years and 10.5 years, respectively. During this period, 70 participants with WCH and 48 normotensive control subjects experienced a fatal or nonfatal CVD event. Systolic WCE increased by 3.83 mm Hg (95% confidence interval [CI]: 3.10 to 4.56 mm Hg) per 10-year increase in age, and was 3.88 mm Hg (95% CI: 0.02 to 7.74 mm Hg) higher in diabetic than in nondiabetic subjects. The incidence of CVD events was significantly higher in the high-risk subjects with WCH compared with the matched high-risk normotensive subjects (hazard ratio [HR]: 2.06; 95% CI: 1.10 to 3.84). Low- risk subjects with WCH and normotensive participants having <3 CVD risk factors were at similar long-term CVD risk (HR: 1.06; 95% CI: 0.66 to 1.72).
In a subgroup analysis of 342 high- and 342 low-risk subjects aged 65 years, older low-risk subjects with WCH (n=250) and their cohort- and age-matched low-risk normotensive control subjects were at similar long-term CVD risk (HR: 0.88; 95% CI: 0.51 to 1.53). The incidence of CVD events after follow-up was significantly higher in the 92 older high-risk subjects with WCH (30 new CVD events) as compared with their high-risk and age-matched normotensive controls (12 new CVD events; HR: 2.19; 95% CI: 1.09 to 4.37).
The authors acknowledged the following limitations: (1) the IDACO database cohorts were limited to a single ABPM procedure and (2) conventional office BP readings taken at the same setting.
The authors concluded that after accounting for age, the size of the WCE was not influenced by the severity of CVD risk or the presence of past CVD events; and that the event rate of new CVD events, after accounting for equal event rates in the WCH and the age-matched normotensive comparative group, was confined to an excess of 22 new CVD events in persons thought to have WCH who were ≥60 years of age at baseline and were at high CVD risk.
Mancia G, Facchetti R, Grassi G, et al. Adverse prognostic value of persistent office blood pressure elevation in white coat hypertension. Hypertension. 2015 Aug;66(2):437-44. Epub 2015 Jun 8. PMID: 26056342.
The aim of this observational cohort study was to stratify cardiovascular risk in white coat hypertension to identify patients in need of closer follow-up and possible antihypertensive drug treatment. The data came from the Pressioni Arteriose Monitorate E Loro Alterazioni (PAMELA) population, which consisted of 2051 people randomly selected from the residents of the Italian town of Monza to be representative of its population for sex, age, age decade, and socioeconomic characteristics, between 1991 and 1993. The participants were followed for a mean of 16 years.
OBPM was measured 3 times by mercury sphygmomanometer after subjects sat for 10 minutes. ABPM was set at 20-minute intervals. WCH was diagnosed as 140 mm Hg systolic or 90 mm Hg diastolic BP with a normal 24-hour mean ABPM. Twenty four-hour BP normality was defined as <125/79 mm Hg based on population norms or a guideline based reading of <130/80 mm Hg. Cause of death was obtained from death certificates. This discussion will be restricted to the analysis based on the <125/79 mm Hg population norms because the result for both groups were similar. Data analysis was restricted untreated participants without WCH at baseline divided into 2 groups according to whether office BP values were 140 mm Hg systolic or 90 mm Hg diastolic BP at both visits (stable WCH) (n=849) or at 1 visit only (unstable WCH) (n=193), compared to patients who were normotensive at baseline (n=132, totaling 1164). The hazard ratio of cardiovascular or all-cause mortality was calculated by the Cox proportional hazard model, with the normotensive group the referent.
Patients with WCH, both stable and unstable, were older and more often male, had higher baseline serum glucose, HDL and total serum cholesterol, and left ventricular mass index. The first visit office SBP for the normotensives, and the unstable and stable WCH patients was 116, 133, and 147 mm Hg, respectively. The DBP was 76, 86, and 89 mm Hg, respectively. The 24-hour ABPMs for all 3 groups was <120/75 mm Hg. During the 16-year follow-up there were 22 cardiovascular and 112 all- cause deaths (Figure 5).
Figure 5 Incidence of cardiovascular (CV) and all-cause mortality in normotensive (NT), unstable white coat hypertension (WCH), and stable WCH subjects
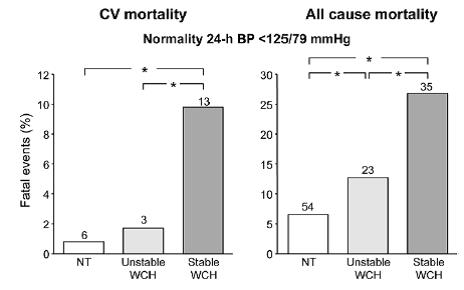
Asterisk refers to the statistical significance (P<0.05) of the between-group differences.
Figure 6. Hazard ratio (HR) of cardiovascular (CV) and all-cause mortality in normotensives (NT), unstable white coat hypertension (WCH), and stable WCH subjects
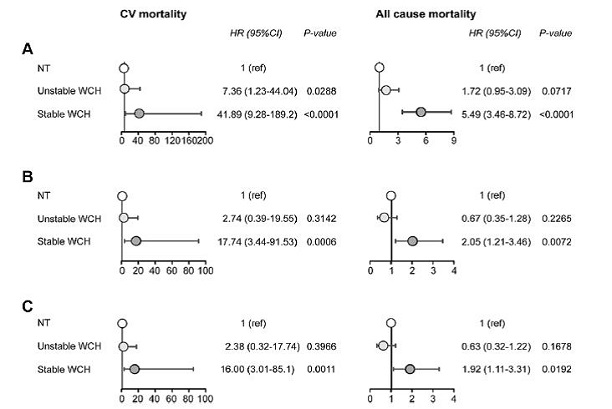
Unadjusted (A), after adjustment for available baseline variables (B) and after further adjustment for 24-hour mean systolic BP (C). Normotensive subjects are the reference (ref).
The results of the Cox proportional hazards model are shown in Figure 6. The risk of cardiovascular and all-cause mortality for 1 SD increase did not differ significantly between normotensive and unstable WCH subjects. In contrast, in stable WCH subjects, the mortality risk was always significantly increased regardless of adjustment for cardiovascular and all-cause mortality in stable WCH.
The authors acknowledged the following limitations: 1) There were only 2 sets of office BP values and one ABPM limiting the chance to observe whether prognosis of WCH individuals is affected also by stability of ABPM normality or OBPM values over a greater number of visits. 2) Their outcomes were limited to fatal events, reducing the statistical power. 3) The authors could not rule out whether antihypertensive drugs were administered during follow-up, which may have had a favorable effect on the incidence of cardiovascular events.
The authors concluded that their results indicate that in-office WCH, and not just out-of-office, BP is an important independent component of the overall risk of this condition.
Cuspidi C, Facchetti R, Bombelli M, et al. Risk of new-onset metabolic syndrome associated with white-coat and masked hypertension: data from a general population. J Hypertens. 2018 Sep;36 (9):1833-1839.
The authors used the observational data from the PAMELA study (see description of PAMELA above, in Mancia et al, 2015) to evaluate whether new-onset metabolic syndrome (MetS) (a syndrome characterized by the clustering of multiple risk factors, such as high-normal or elevated BP, hyperglycemia, low high-density cholesterol, elevated triglycerides and abdominal obesity) was related OBPM and ABPM. Participants were divided into four groups for the analysis: [1] normal OBPM (<140/90 mm Hg) and ABPM (<130/80 mm Hg); [2] elevated office SBP or DBP and normal ABPM (WCH); [3] normal OBPM and elevated 24-hour SBP or DBP (masked hypertension; and [4] elevated OBPM and 24-hour SBP or DBP (sustained hypertension).
The diagnosis of MetS was based on the presence of 3 or more of the following: office SBP 130 mm Hg or higher and/or DBP 85 mm Hg or higher or use of an antihypertensive drug; waist circumference at least 102 cm (men) or at least 88 cm (women); serum triglycerides at least 150 mg/dl; serum HDL cholesterol (HDL-C) 40 mg/dl or less (men) or 50 mg/dl or less (women); and fasting blood glucose at least 110 mg/dl or use of antidiabetic medications. The authors calculated the incidence of MetS as the presence of MetS at second examination in participants without the MetS at baseline. They used multiple logistic regression to evaluate the relationship between demographic and clinical variables and new-onset MetS and its components.
The analysis included 1182 participants without MetS at baseline and with measurable variables of interest at follow-up examination performed 10 years later, 108 (8.8%) of whom developed MetS at the follow up examination. Note: 326 of 2024 participants had MetS at baseline and were not included. Compared with normotensive participants, participants with WCH, masked hypertension and sustained BP were more likely to be male (44.9% vs. 56.8%, 60.5%, and 61.1%, respectively), older (mean of 44, vs. 50.4, 49.5, and 58.7, respectively), have a mean larger waist circumference (80.3 cm vs. 86.4, 86, and 88.2, cm, respectively), higher mean blood glucose (84.8 mg/dl vs. 91, 86.1, and 90.6 mg/dl, respectively), and mean triglycerides (89.5 mg/dl vs. 104.2, 105.9, and 101.9 mg./dl, respectively). They also had higher mean office based SBP (117.4 mm Hg, vs. 139.9, 125.5, and 155 mm Hg, respectively) and DBP (77 mm Hg, vs. 91, 80.7, and 94.6 mm Hg, respectively); and higher mean 24-hour SBP (113.8 mm Hg, vs. 120.9, 123.6, and 131.5 mm Hg, respectively), and DBP (71.2 mm Hg vs. 76.3, 76.7, and 81.2 mm Hg, respectively). All of these differences were statistically significant.
There was a statistically significant greater unadjusted incidence of new-onset MetS was in each hypertensive group when BP was defined by ABPM compared to OBPM. After adjustment for age and sex, the risk related to WCH (OR 2.03, 95% CI 1.21–3.41), masked hypertension (OR 2.55, 95% CI 1.26–5.17) and sustained hypertension (OR 2.28, 95% CI 1.43–3.99) defined by ABPM vs. OBPM criteria. The authors also evaluated out-of-office BP and found it not to be consistently related to MetS.
The authors acknowledged the following limitations: 1) The findings were from a middle-age population with a relatively low prevalence of MetS, obesity, diabetes, as well as a 10-year incidence of MetS of less than 10%, making extrapolation to other populations difficult; 2) Data about level of physical activity were unavailable in the PAMELA population; and 3) Participants on antihypertensive therapy were not excluded from our study, to reflect real world conditions at population level.
The authors concluded that 24-hour ABPM is a key correlate of new-onset MetS, but that OBPM and HBPM are not. In addition, they conclude that a comprehensive evaluation of BP status based on office/ambulatory measurements may substantially improve risk stratification of new-onset MetS (and single components such as abdominal adiposity and hyperglycemia) and prevention strategies.
Tientcheu D, Ayers C, Das SR, et al. Target Organ Complications and Cardiovascular Events Associated With Masked Hypertension and White-Coat Hypertension: Analysis From the Dallas Heart Study. J Am Coll Cardiol. 2015 Nov 17;66(20):2159-2169.
The aim of this study was to evaluate target organ damage and adverse cardiovascular outcomes associated with WCH, masked hypertension, and sustained hypertension in the DHS (Dallas Heart Study). The DHS was a multiethnic probability-based population sample of Dallas County, established in 2000, designed to oversample African Americans. The resulting cohort was 54% African American and 49% women.
Of the initial 6,101 participants, aged 30 to 65 years of age, 3,557 agreed to a second in-home visit and 3,027 completed a third study visit at UT Southwestern Medical Center, where OBPM was measured. OBPM was conducted in the same fashion as during the in-home visit, using the same oscillometric device. During the clinic visit, magnetic resonance imaging (MRI) was performed to assess aortic pulse wave velocity (APWV). ABPM was not used.
The average of the third to fifth BP measurement was used as the home BP and clinic BP. WCH was defined home BP <135/85 mm Hg and clinic BP ≥140/90 mm Hg. Masked hypertension was home BP ≥135/85 mm Hg and clinic BP <140/90 mm Hg; sustained hypertension home BP ≥ 135/85 mm Hg and clinic BP ≥140/90 mm Hg; and normotension as normal home and clinic BP. Presence of CKD was defined as estimated GFR <60 ml/min/1.73 m2 or urinary albumin to creatinine ratio of at least 17 mg/g in women or 25 mg/g in men. The number of classes of antihypertensive drugs was defined as the number of drugs being taken. The authors also measured cystatin C to indicate chronic kidney disease, and aortic arch pulse wave velocity as an indicator of arterial stiffness. Adjudicated CVD events included: unstable angina; myocardial infarction; coronary artery bypass grafting; percutaneous coronary intervention; stroke; transient ischemic attack; cerebrovascular revascularization; hospitalization for atrial fibrillation or heart failure; and cardiovascular death.
The associations of WCH, masked hypertension and sustained hypertension with clinical endpoints were evaluated using multivariable Cox proportional hazards regression models. Subjects with a history of cardiovascular disease at baseline were excluded from the analysis (n = 227). Subjects without a clinical endpoint that were lost to follow-up for nonfatal events were censored at the time of last contact (n = 64, median follow up 5.0 years).
The sample weight-adjusted prevalence of WCH, masked hypertension, and sustained hypertension were 3.3%, 17.8%, and 12%, respectively. In untreated participants, the prevalence was 2.2%, 13.6%, and 7.8%, respectively. Compared to normotensive participants, those with WCH, masked hypertension, and sustained hypertension were more likely to be black (41.7%, 63.4%, 55.8%, and 68.9%, respectively), older (mean age = 40, 49, 47, and 50 yrs., respectively), more obese (mean BMI = 28, 31, 31, and 32 kg/m2, respectively), on antihypertensive medications (12.8%, 35.0%, 29.6%, and 39.1%, respectively), to have chronic kidney disease, and/or cardiovascular diseases (Figure 7).
Figure 7. Markers of Subclinical Vascular and Renal Damage among Participants with WCH, masked hypertension (MH), sustained hypertension (SH), and normotensives (NT)
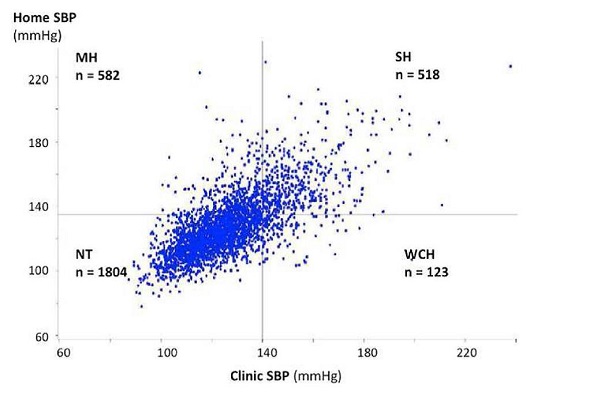
There were 47 cardiovascular deaths and 194 composite cardiovascular events over a median follow- up of 9.4 years. In the survival analysis, after adjusting for age, sex, and race/ethnicity, BMI, diabetes mellitus, smoking, and total cholesterol levels (model 1), WCH was independently associated with higher cardiovascular risk compared with the normotensive group (HR 2.09, 95% CI: 1.05 to 4.15). The association of WCH with cardiovascular events remained significant in the model after adjustment for both traditional cardiovascular risk factors and antihypertensive medication treatment (Model 3, Table 8). After adjustment for both self-reported history of hypertension and prevalent antihypertensive treatment in Model 4, the association of WCH with composite cardiovascular events was positive but not significant. Similarly, masked hypertension was associated with increased cardiovascular risk compared with the NT group after adjustment of traditional risk factors (adjusted HR: 2.03, 95% CI: 1.36 to 3.03), and in all models that accounted for both self-reported history of hypertension and antihypertensive treatment.
| Table 8. Adjusted HRs for Composite Cardiovascular Events Associated With Each Hypertension Classification Compared With Participants With Normal BP |
|---|
| BP Categories |
# of Events |
Events/100 Person-Yrs |
Unadjusted HR (95% CI) |
HR (95% CI) Model 1 |
HR (95% CI) Model 2 |
HR (95% CI) Model 3 |
HR (95% CI) Model 4 |
| Nomrotensive |
52 |
0.37 |
reference |
reference |
reference |
reference |
reference |
| White coat hypertension |
10 |
1.10 |
3.09
(1.57-6.08) |
2.09
(1.05-4.15) |
1.99
(1.00-3.97) |
2.01
(1.01-3.99) |
1.98
(0.99-3.95) |
| Masked hypertension |
53 |
1.24 |
3.41
(2.33-4.99) |
2.03
(1.36-3.03) |
1.65
(1.05-2.61) |
1.93
(1.29-2.89) |
1.84
(1.17-2.88) |
| Sustained hypertension |
79 |
2.18 |
6.52
(4.62-9.21) |
3.12
(2.13-4.56) |
2.37
(1.48-3.79) |
2.87
(1.96-4.20) |
2.68
(1.68-2.28) |
| Model 1: age, sex, race, BMI, diabetes, smoking, serum cholesterol level. Model 2: model 1 + hypertension. Model 3: model 1 + treatment for hypertension. Model 4: model 1 + hypertension + treatment for hypertension |
| BP = blood pressure; CI = confidence interval; HR = hazard ratio |
The authors acknowledged a number of limitations to their study. First, there was a relatively small number of participants with WCH. Although cardiovascular risk associated with WCH in nonblack patients was lower than in black patients, there was not adequate statistical power to evaluate the interaction between race and the impact of WCH. Second, they could not exclude the possibility that treatment of hypertension between the home and clinic visits may have led to normalization of office BP and over diagnosis of masked hypertension. Third, the rates of progression to sustained hypertension among individuals with WCH and masked hypertension are unknown because home BP was not measured during the follow-up study. Fourth, out-of office BP was obtained by surveyors, rather than by participants, which may not truly reflect out of office BP. Fifth, the statistical analysis study was not adjusted for multiple testing between WCH, MH, and SH versus control groups.
The authors concluded that masked hypertension was common in their cohort, occurring in 18% of participants overall and in 14% of those not receiving antihypertensive treatment, comprising >50% of the prevalent hypertension cases in the cohort. They concluded that both WCH and masked hypertension were associated with markers of increased aortic stiffness and renal damage, as evidenced by albuminuria and higher cystatin C levels. Finally, both WCH and masked hypertension were associated with increased cardiovascular events in a multiethnic, probability-based population sample of Dallas county adults.
Huang Y, Huang W, Mai W, Cai X, An D, Liu Z, Huang H, Zeng J, Hu Y, Xu D. White-coat hypertension is a risk factor for cardiovascular diseases and total mortality. J Hypertens. 2017 Apr;35(4):677-688. doi: 10.1097/HJH.0000000000001226. Review. PMID: 28253216; PubMed Central PMCID: PMC5338886.
This was a meta-analysis aimed at evaluating the inconsistencies across studies of WCH and its association with CVD and all-cause mortality. Using the methodology described by Stroup et al. (2000) for the meta-analysis of observational data, the authors searched PubMed, EMBASE, CINAHL Plus, Scopus, and Google Scholar for prospective cohort studies to 31 August 2016.
Studies included were prospective studies with: adult participants with assessment of WCH on the risks of CVD or all-cause mortality; and multivariate-adjusted relative risks (RRs) or hazard ratios and 95% confidence intervals (CIs) for events associated with WCH compared with normotension individuals. WCH was defined as high-clinic BP but normal out-of-office BP based on ABPM or HBPM. Normotension was defined as normal BP in both clinic and out-of-office settings. Studies were excluded if enrollment depended on having a particular condition or risk factor such as chronic kidney disease or diabetes mellitus.
The authors based their quality assessment on the Newcastle–Ottawa Quality Assessment Scale (NOS) for cohort studies (Huang et al., 2016), in which studies are judged on three broad perspectives as follows: selection (four items, one star each), comparability (one item, up to two stars), and exposure/outcome (three items, one star each). The authors evaluated whether the studies were adequately adjusted for potential confounders: age; sex; previous CVD or exclusion of CVD at baseline; diabetes mellitus or fasting plasma glucose; BMI; cholesterol or hypercholesterolemia; and smoking.
The primary and secondary outcomes were the risk of CVD and all-cause mortality, respectively. There were three stratification analyses: 1) the risks of CVD and all-cause mortality in people with WCH not treated for high BP (‘untreated’) vs. normotensives; 2) the risks of CVD and all-cause mortality in people on high treatment (‘treated’) vs. patients whose BP was normalized after medication; and 3) the risks of CVD and all-cause mortality in a mixed population with WCH who were either on or without high BP treatment vs. normotensives or hypertension patients whose BP was normalized after treatment.
After screening more than 26,000 articles, the authors identified 62 that qualified for full review. Fourteen articles were included in the meta-analysis. In the analysis of CVD risk, these included 8 studies consisting of 23 cohorts, totaling 20,445 people with mean follow-up of 9.6 years; 4 studies consisting of 11 cohorts, totaling 8656 people with mean follow-up of 5.3 years; and 6 studies consisting of 12 cohorts, totaling 21,336 people with mean follow-up duration of 8.2 years were included in untreated, treated, and mixed populations comparisons, respectively. In the analysis of all-cause mortality, there were 4 studies totaling 15,793 people with mean follow-up duration of 10.9 years included for the meta-analysis of the untreated population. Because there was only one study each of treated and mixed population, these data were not meta-analyzed. Ten studies were graded as good, and four studies as fair. The two fair studies were not adequately adjusted for potential confounders.
The WCH patients in untreated, treated, and mixed population had 27.6, 21.9, and 27.3 mm Hg higher office SBP, and 12.6, 9.8, and 12.1 mm Hg higher clinic DBP than their corresponding normotension comparators, respectively. Using fixed-effects models, after multivariable adjustment, WCH was associated with significantly increased risk of CVD in untreated patients (RR 1.38, 95% CI 1.15–1.65) and mixed populations (RR 1.19, 95% CI 1.01–1.41). The risk did not reach statistical significance in treated patients with WCH compared with patients whose BP had been normalized by medication (RR 1.16, 95% CI 0.91–1.49).
Figure 8. Forest plot: white-coat hypertension vs. normotension and outcome: cardiovascular disease.
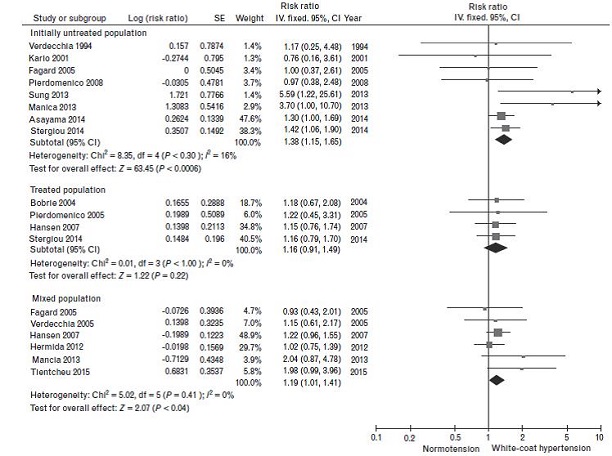
In the subgroup analyses (Table 9), in untreated patients, WCH was significantly associated with higher risk of CVD in both subgroups of ABPM or other out-of-office BP measurement, either participant’s age less than 55 or at least 55 years, studies with fatal CVD or fatal and nonfatal CVD. Increased risk of CVD was also found in subgroups with WCH defined as daytime ABPM less than 135/85 mm Hg, follow-up duration at least 8 years, adequate adjustment of confounders, or good study quality. In the mixed populations, the risk of CVD was significantly increased in subgroups with WCH, follow-up duration at least 8 years, adequate adjustment of confounders, and good study quality. In treated subgroups, all analyses indicated that WCH was not associated with the risk of CVD.
| Table 9: Subgroup analyses of the association between white-coat hypertension and risk of cardiovascular disease |
|---|
| |
|
Untreated population |
Treated population |
Mixed population |
| Subgroups |
Number of studies |
RR (95% CI) |
Number of studies |
RR (95% CI) |
Number of studies |
RR (95% CI) |
| Measurement of out-of-office BP |
|
|
|
|
|
|
| |
ABPM |
6 |
1.34(1.07,1.69) |
2 |
1.16(0.79,1.70) |
5 |
1.15(0.96,1.37) |
| |
HBPM |
1 |
1.41(1.06,1.90) |
2 |
1.17(0.85,1.60) |
2 |
2.25(1.30,3.92) |
| Thresholds for ABPM |
|
|
|
|
|
|
|
| |
Daytime ABP < 135/85 mmHg |
4 |
1.36(1.08,1.72) |
2 |
1.16(0.79,1.70) |
3 |
1.13(0.94,1.35) |
| |
24-h ABP < 130/80 mmHg |
2 |
1.19(0.92,1.52) |
0 |
- |
0 |
- |
| |
Others |
1 |
1.17(0.25,5.48) |
0 |
- |
2 |
1.37(0.78,2.40) |
| Measurement of clinic BP |
|
|
|
|
|
|
|
| |
≥ 2 visits |
3 |
0.96(0.47,1.96) |
2 |
1.16(0.87,1.53) |
1 |
1.98(0.99,3.96) |
| |
< 2 visist |
5 |
1.45(1.20,1.74) |
2 |
1.19(0.73,1.95) |
5 |
1.16(0.97,1.37) |
| Follow-up duration |
|
|
|
|
|
|
|
| |
< 8 years |
3 |
0.96(0.47,1.96) |
2 |
1.19(0.73,1.95) |
2 |
1.04(0.79,1.38) |
| |
≥ 8 years |
5 |
1.45(1.20,1.74) |
2 |
1.16(0.87,1.53) |
4 |
1.29(1.05,1.59) |
| Average age |
|
|
|
|
|
|
|
| |
< 55 years |
5 |
1.45(1.15,1.83) |
0 |
- |
3 |
1.20(0.92,1.57) |
| |
≥ 55 years |
3 |
1.35(1.03,1.79) |
3 |
1.17(0.87,1.59) |
3 |
1.19(0.96,1.47) |
| CVD endpoint |
|
|
|
|
|
|
|
| |
Fatal CVD |
2 |
3.61(1.88,6.95) |
0 |
- |
1 |
2.04(0.87,4.78) |
| |
Fatal and nonfatal CVD |
6 |
1.31(1.09,1.57) |
3 |
1.16(0.91,1.49) |
5 |
1.17(0.98,1.39) |
| Adjustment of confounders |
|
|
|
|
|
|
|
| |
Adequate |
7 |
1.42(1.19,1.70) |
4 |
1.16(0.91,1.49) |
5 |
1.28(1.04,1.56) |
| |
Not adequate |
1 |
0.76(0.16,3.61) |
0 |
- |
1 |
1.02(0.75,1.39) |
| Study quality |
|
|
|
|
|
|
|
| |
Good |
6 |
1.43(1.19,1.72) |
3 |
1.16(0.90,1.49) |
5 |
1.28(1.04,1.56) |
| |
Fair |
2 |
1.02(0.46,2.27) |
1 |
1.22(0.45,3.31) |
1 |
1.02(0.75,1.39) |
| RR=relative risk |
| Adequate adjustment denoted adjustment of at least: age, sex, previous CVD or exclusion of CVD at baseline; diabetes mellitus or fasting plasma glucose; BMI; cholesterol or hypercholesterolemia; and smoking |
In the four studies with all-cause mortality in untreated WCH patients, fixed-effects analysis indicated that the risk of all-cause mortality was increased in the untreated WCH (RR 1.20, 95% CI 1.03–1.40) compared with normotensive patients.
The authors concluded that their evidence implicates WCH as a risk factor for long-term adverse outcomes and that close follow-up should be performed in WCH patients.
Palla M, Saber H, Konda S, Briasoulis A. Masked hypertension and cardiovascular outcomes: an updated systematic review and meta-analysis. Integr Blood Press Control. 2018 Jan 5;11:11-24.
This meta-analysis explored the outcomes of masked HTN in treated and untreated groups of patient populations. The authors searched PubMed, Embase, and Cochrane Central Register of Controlled Trials and found 1553 articles. After deduplication, screening of titles and abstracts, and full-text review based on inclusion and exclusion criteria, nine studies were identified and included in the meta-analysis. Pooled effect of intervention was measured using odds ratios (OR) or standardized mean differences (SMD) with 95% confidence intervals (CI). Mantel–Haenszel fixed-effects models were used to estimate the pooled effect measure if the heterogeneity was <25%. Sensitivity analyses were performed by eliminating each study at a time to assess the influence of any included study on the results and the robustness of results.
There were a total of 14,729 participants (11,245 normotensives, 3484 with masked HTN, 1984 with WCH, and 5143 participants with sustained hypertension (SH)) were included in the meta-analysis. The mean age of the study population was 58 years. The mean follow-up was 9.5 years.
Untreated patients
Composite cardiovascular events occurred in 12.3% of untreated patients with masked HTN and 5.1% of patients with normotension (OR 2.91, 95% CI 2.54–3.33) (Figure 9a). No significant heterogeneity was seen among studies. All-cause death occurred in 15.8% of patients with masked HTN and 7.8% of patients with normotension (OR 2.65, 95% CI 2.18–3.23) (Figure 9b). The patients with masked hypertension were more likely to have cardiovascular events than patients with WCH (12.8% vs. 10.8%, respectively, OR 1.38, 95% CI 1.04–1.83) and all-cause mortality (OR 1.71, 95% CI 1.34–2.19). However, they were less likely to have cardiovascular events than patients with sustained hypertension (OR 0.68, 95% CI 0.53–0.86). There were significant differences in all-cause mortality between patients with masked hypertension and sustained hypertension.
Figure 9a
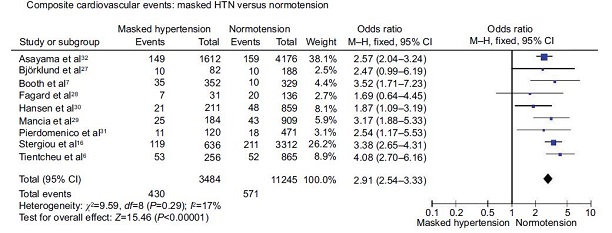
Figure 9b
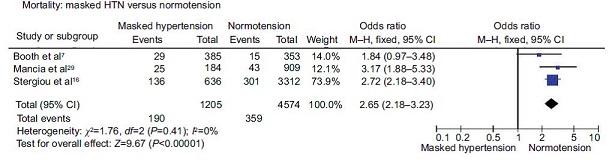
Treated patients
Composite cardiovascular events occurred in 27.9% of patients with masked hypertension and 15.5% of patients with normotension (OR 2.03, 95% CI 1.52–2.72) and all-cause mortality occurred in 15.2% of patients with masked hypertension and 10.4% of patients with normotension (OR 1.44, 95% CI 1.03–2.01). Composite cardiovascular events occurred in 27.9% of patients with masked hypertension and 19.4% of patients with WCH (OR 1.64, 95% CI 1.20–2.25), and there was no significant difference in all-cause mortality between patients with patients with masked hypertension and patients with WCH (21.0% vs. 17.3%, OR 1.03, 95% CI 0.55–1.90).
The authors concluded that, in their meta-analysis of 14,729 patients, cardiovascular morbidity and mortality associated with masked hypertension was higher than normotension and white-coat hypertension but lower than sustained hypertension. Among treated patients, masked hypertension and sustained hypertension were associated with similar rates of cardiovascular events and mortality.
Pediatric hypertension
Iturzaeta A, Pompozzi L, Casas Rey C, et al. Prevalence of masked hypertension among children with risk factors for arterial hypertension. Arch Argent Pediatr. 2018 Oct 1;116(5):328-332. PMID: 30204983.
The aim of this study is to estimate the prevalence of masked hypertension, isolated nocturnal hypertension, and prehypertension in children with risk factors for arterial hypertension. An observational, cross-sectional study conducted at a hospital in Buenos Aires, Argentina recruited consecutive children aged 5 to 11 years with normal blood pressure and at least one risk factor for arterial hypertension. The risk factors for hypertension were divided into neonatal history (such as prematurity, low birth weight, and intrauterine growth restriction), personal history (such as isolated high blood pressure, overweight/obesity, dyslipemia, chronic steroid administration, increased salt intake and diabetes), and family history (such as family hypertension, early cardiovascular events, and diabetes)
If a normal blood pressure was confirmed, a 24-hour ABPM was done. Masked hypertension was defined as an average ambulatory systolic blood pressure (SBP) and / or diastolic blood pressure (DBP) during the day or while doing an activity greater than the 95th percentile by gender and height. Isolated nocturnal hypertension (INH) was defined as an average ambulatory blood pressure during the day or while doing an activity below the 95th percentile and nighttime values greater than the 95th percentile by sex and height. For the descriptive analysis, absolute numbers and proportions with their corresponding 95% confidence interval (95% CI) were used for categorical outcome measures and mean or median with standard deviation or quartiles were used for continuous outcome measures, based on their adjustment or not to normality. The absolute number of patients with masked hypertension (numerator) divided by the total number of screened patients (denominator) multiplied by 100 was used to estimate the prevalence of masked hypertension as a percentage.
One hundred and ten patients with an average age of 8.7 ± 1.8 years were included; 55% were girls. ABPM average duration was 23.18 ± 1.8 hours. Average body mass index (BMI) was 22.6 ± 5.5. Twenty-three patients had neonatal history; all had at least one risk factor for arterial hypertension corresponding to personal history with the most common ones being increased salt intake followed by obesity; 101 had at least one risk factor corresponding to family history. Considering a pool of the 3 types of history (neonatal, personal, and family), 65 patients had between 7 and 10 risk factors.
The ABPM was performed in the 110 participants. Average 24 hour systolic blood pressure was 109.3 ± 8.7 mmHg and diastolic blood pressure was 65.7 ± 5.8 mmHg. ABPM identified 10 patients with masked hypertension (9.1%; 95% confidence interval [CI]: 5.1-15.9) and seven had isolated nocturnal hypertension (6.4%; 95% CI: 3.1-23.5). The analysis of patients with masked hypertension (n=10) showed that seven boys, and nine obese or overweight children had at least one risk factor for hypertension corresponding to family history. The average 24-hour, daytime, and nighttime systolic blood pressure, diastolic blood pressure, and mean blood pressure (MBP) values (ABPM) of patients with masked hypertension were higher than those of patients with a normal ABPM.
The authors acknowledged the following limitations: the study was not designed to establish risk factors but to estimate the prevalence of masked hypertension and prevented any statistical analysis of inference leading to potential type II error, a mistaken failure to reject the null hypothesis when the alternative hypothesis is true and there is a real association between two factors.
The authors concluded that the prevalence of masked hypertension in children who had at least one risk factors for arterial hypertension was 9.1%. The prevalence of isolated nocturnal hypertension was 6.4%.
Nocturnal hypertension
Hermida RC, Crespo JJ, Otero A, et al. Asleep blood pressure: significant prognostic marker of vascular risk and therapeutic target for prevention. Eur Heart J. 2018 Dec 14;39(47):4159-4171.
The aim of the study was to prospectively investigate whether with treatment-induced changes in ABPM-derived parameters such as a progressive decrease of either office, ambulatory awake, or asleep blood pressure mean is associated with cardiovascular disease risk reduction. The prospective multicenter Hygia Project is a research network established to extend the use of ABPM in primary care to diagnose hypertension, evaluate response to treatment, and assess patient cardiovascular disease and other risks. The Hygia Project was composed of 40 primary care centers in Northern Spain and involves 292 investigators properly trained to ABPM. The study population consisted of Spanish men and women ≥18 years of age, adhering to a routine of daytime activity and night-time sleep, referred for ABPM mainly to confirm/refute the diagnosis of hypertension inferred by daytime office blood pressure measurement (OBPM) of untreated individuals or to evaluate blood pressure control in treated hypertensive persons.
Ambulatory BP was measured every 20 minutes between 07:00 and 23:00 hours and every 30 minutes during the night for 48 consecutive hours. Awake and asleep ambulatory blood pressure means were calculated using all valid readings of the actual hours, respectively, of daytime activity and night-time sleep as differentiated by participant diary entries. The respective 48 hour, awake, and asleep BP means were then determined as the average of the corresponding blood pressure means obtained for each time-class. Participants were designated as dipper if the sleep-time relative SBP decline was ≥10%, and as non-dipper otherwise. Hypertension was defined according to current ABPM criteria as awake systolic blood pressure (SBP)/diastolic blood pressure (DBP) mean ≥135/85 mmHg, or asleep SBP/DBP mean ≥120/70 mmHg, or on blood pressure lowering treatment. Diabetes was defined as fasting glucose ≥126 mg/dL on at least two clinical assessments ≥3 months apart in participants without prior history of diabetes, or glucose-lowering treatment.
Investigators, mainly those of the Hygia Project Scientific Committee, reviewed the complete electronic clinical records of every enrolled participant at least annually and at least 1 year following each person’s last ABPM evaluation. Categorization of CVD and other events listed in the electronic clinical records was accomplished by previously defined diagnostic criteria at the corresponding referring tertiary hospital services and by external non-investigator medical specialists. The Hygia Project Events Committee, composed of independent clinicians blinded to medical records, participant’s identification, ABPM findings, and treatment scheme of those with hypertension, evaluated clinical reports to ascertain and certify every documented event. Documented events included death from all causes, myocardial infarction, angina pectoris, coronary revascularization, heart failure, lower extremities acute arterial occlusion, retinal artery thrombotic occlusion, hemorrhagic stroke, ischemic stroke, and transient ischemic attack. The a priori defined primary vascular study endpoint was cardiovascular disease outcome, a composite of CVD death, myocardial infarction, coronary revascularization, heart failure, ischemic stroke, and hemorrhagic stroke. The Cox proportional-hazard model, adjusted for significant confounding variables, served to estimate hazard ratios (HR) and 95% confidence interval (CI) for events per tested potential prognostic blood pressure parameter as well as their combinations. The hazard ratio was standardized by expressing them in terms of 1-SD increments of the blood pressure parameter. All demographic, anthropometric, and clinical laboratory variables were tested as potential confounding variables by non-automatic forward and backward stepwise Cox survival analysis.
During the 5.1-year median follow-up period, 2311 individuals had any event, including 1209 experiencing the primary outcome which was a composite of cardiovascular disease death, myocardial infarction, coronary revascularization, heart failure, and stroke. A total of 18,078 individuals, 59.1± 14.3 (mean ± standard deviation [SD]) years of age and 54% men, were prospectively evaluated with baseline ambulatory blood pressure with 15,674 participants defined as having hypertension. Body mass index (BMI) was 29.6 kg/m2 and 21.3% had type 2 diabetes, 42.5% had obesity, and 24.7% had chronic kidney disease. Event-subjects were predominantly men, of older age, and at baseline were likely to have type 2 diabetes, metabolic syndrome, anemia, chronic kidney disease, and/or history of previous CVD event. The mean 48 hour systolic blood pressure was 128.6 mm Hg, the mean 48 hour diastolic blood pressure was 75.7 mm Hg, the mean asleep systolic blood pressure was 119.9 mm Hg, the mean asleep diastolic blood pressure was 68.0 mm Hg, and 46.4% were non-dippers. These five ABPM parameters were statistically significantly different comparing participants with no event to participants with events.
| Table 10 Adjusted HR of CVD outcome associated with OBPM and ABP |
|---|
|
| OBPM/ABPM parameter |
Baseline BP |
Final BP |
Follow up Decrease in BP |
|---|
|
| SBP |
|---|
Office |
1.19 (1.14–1.26)* |
1.15 (1.09–1.21)* |
0.85 (0.77–0.93)* |
Awake mean |
1.20 (1.14–1.26)* |
1.25 (1.19–1.31)* |
0.78 (0.71–0.86)* |
Asleep mean |
1.34 (1.27–1.40)* |
1.31 (1.25–1.37)* |
0.75 (0.69–0.82)* |
48 h mean |
1.26 (1.20–1.32)* |
1.28 (1.22–1.34)* |
0.77 (0.70–0.84)* |
| Sleep-time relative decline |
0.81 (0.77–0.85)* |
0.86 (0.82–0.91)* |
1.21 (1.11–1.32)* |
SD, awake |
1.25 (1.19–1.31)* |
1.23 (1.17–1.29)* |
0.99 (0.91–1.09) |
SD, asleep |
1.09 (1.04–1.15)* |
1.10 (1.05–1.16)* |
0.92 (0.85–1.03) |
SD, 48 h |
1.14 (1.08–1.20)* |
1.16 (1.10–1.22)* |
1.05 (0.96–1.16) |
Morning surge |
0.92 (0.87–0.97)* |
0.94 |
0.94 (0.85–1.04) |
Pre-awakening surge |
0.87 (0.83–0.92)* |
0.93 |
1.10 (0.99–1.22) |
Sleep-time fall |
0.96 (0.91–1.01) |
0.96 (0.91–1.01) |
1.15 (1.05–1.27)** |
| DBP |
|---|
Office |
1.07 (1.00–1.13)*** |
1.07 |
0.89 (0.81–0.98)*** |
Awake mean |
0.99 (0.93–1.06) |
1.09 |
0.88 (0.79–0.98)*** |
Asleep mean |
1.17 (1.10–1.23)* |
1.20 (1.14–1.27)* |
0.76 (0.69–0.84)* |
48 h mean |
1.06 (0.99–1.13) |
1.14 (1.07–1.21)* |
0.83 (0.75–0.92)* |
| Sleep-time relative decline |
0.81 (0.77–0.86)* |
0.85 (0.81–0.90)* |
1.29 (1.18 –1.42)* |
SD, awake |
1.18 (1.12–1.24)* |
1.18 (1.11–1.24)* |
0.93 (0.84–1.01) |
SD, asleep |
1.07 (1.01–1.13)*** |
1.06 |
1.00 (0.91–1.10) |
SD, 48 h |
1.03 (0.98–1.10) |
1.07 |
1.09 (0.98–1.20) |
Morning surge |
0.95 (0.90–1.00) |
0.94 |
1.06 (0.96–1.18) |
Pre-awakening surge |
0.88 (0.83–0.93)* |
0.89 (0.84–0.94)* |
1.17 (1.06–1.30)** |
|
|
CVD outcome: Composite of CVD death, myocardial infarction, coronary revascularization, heart failure, ischaemic stroke, and haemorrhagic stroke.
Baseline and final BP evaluation: Standardized adjusted HRs (95% CI) expressed per 1-SD elevation in each evaluated BP parameter either at the baseline evaluation upon recruitment (left column) or at the last available evaluation per participant (centre column). For the individualized analysis of each listed BP parameter, adjustments were always applied for significant influential characteristics of age, sex, diabetes, CKD, cigarette smoking, HDL-cholesterol, hypertension treatment-time, and history of previous CVD event.
Decrease during follow-up: Standardized adjusted HRs (95% CI) expressed per 1-SD decrease in each evaluated BP parameter during follow-up (right column). For the individualized analysis of each listed BP parameter, adjustments were applied for significant influential characteristics of age, sex, diabetes, CKD, cigarette smoking, HDL-cholesterol, baseline values of the tested BP parameter, hypertension treatment-time, and history of previous CVD event. Decrease in BP at each ABPM evaluation from baseline was entered as a time-dependent covariate in the Cox regression models.
Sleep-time relative BP decline, index of BP dipping, is defined as percent decline in BP during night-time sleep relative to mean BP during daytime activity, and calculated as: [(awake BP mean - asleep BP mean)/awake BP mean] 100. Morning BP surge was calculated as difference between average BP during first 2 h after morning wake-up (i.e. morning BP) and hourly BP average centred on lowest BP reading recorded during night-time sleep (i.e. lowest sleep BP). Pre-awakening BP surge was calculated as difference between average BP during first 2 h after and average BP during 2 h just before morning wake-up. Sleep-time fall was calculated as difference between average BP during the 2 h just before going to bed and hourly average centred on lowest BP reading recorded during night-time sleep.
*P < 0.001.
**P < 0.01.
***P < 0.05.
|
|
The largest difference between the event and non-event cohorts was in the asleep systolic blood pressure mean. Prevalence of non-dipping was significantly higher, 66 vs. 44%, among event subjects (p < 0.001). The asleep systolic blood pressure (SBP) mean was the most significant blood pressure-derived risk factor for the primary outcome (HR 1.29, [95% CI] 1.22–1.35 per SD]elevation; P < 0.001), regardless of office blood pressure (HR 1.03, 95% CI 0.97–1.09; P = 0.32), and awake SBP (HR 1.02, 95% CI 0.94–1.10, p = 0.68). The asleep systolic blood pressure mean was the most significant blood pressure marker of cardiovascular disease risk [per 1-SD elevation, adjusted HR 1.34 (95% CI 1.27–1.40), P < 0.001), as shown in Table 2. But a greater either morning or preawakening BP surge calculated as previously defined was significantly associated with lower, not higher, CVD risk. The merit of the asleep SBP mean as marker of CVD risk was highly statistically significant independent of absence/presence of hypertension therapy at baseline [HR 1.30 (95% CI 1.18–1.42), P < 0.001; and 1.31 (95% CI 1.24–1.38), P < 0.001, respectively]. Most importantly, the progressive attenuation of asleep SBP was the most significant marker of event-free survival (HR 0.75, 95% CI 0.69–0.82 per SD decrease; P < 0.001), regardless of changes in office blood pressure mean (HR 1.07, 95% CI 0.97–1.17; P = 0.18], or awake SBP mean (HR 0.96, 95% CI 0.85–1.08; P = 0.47) during follow-up. Only the decrease in asleep SBP mean and increase in sleep-time relative SBP decline towards the more normal dipper BP pattern remained jointly and significantly associated with reduced CVD risk. There was a highly statistically significant exponential decrease in risk of CVD outcome with progressively lower achieved asleep SBP mean after treatment.
The authors acknowledged the following limitations: (i) the findings require validation and extrapolation to other ethnic groups; (ii) OBPM was obtained in the presence of the investigator and thus potentially overestimated, although their approach reflects current medical practice as utilized in most previously reported studies; and (iii) with regard to the potential increase in CVD event-free survival time with progressive decrease in asleep SBP mean, a confirmatory study randomizing participants to at least two different threshold goals in terms of achieved asleep SBP mean is required to properly validate their findings.
The authors concluded that asleep systolic blood pressure (SBP) was the most significant prognostic ABPM-derived risk factor for cardiovascular outcomes, stronger than OBPM or any other ABPM-derived parameter. Further, changes in ABPM parameters during follow-up documented the progressive decrease in asleep systolic BP mean and increase in sleep-time relative systolic BP decline towards the more normal dipper BP pattern were significantly associated with reduced CVD risk. Thus, the sleep-time relative SBP decline, and not just the dipping classification per se usually based on an arbitrary 10% threshold value, might be used, jointly with the asleep systolic BP level, as novel clinical indices to assess and prevent risk for future major CVD events. They also found a greater morning or preawakening BP surge was significantly associated with lower, not higher, CVD risk. The authors concluded that around-the-clock ambulatory blood pressure monitoring should be recommended to derive the asleep systolic BP to diagnose true hypertension.
Xie JC, Yan H, Zhao YX, et al. Prognostic value of morning blood pressure surge in clinical events: a meta-analysis of longitudinal studies. J Stroke Cerebrovasc Dis. 2015 Feb;24(2):362-9.
The aim of the study was conducted to summarize the prognostic significance of morning blood pressure surge (MS) in predicting future cardiovascular (CV) events by comparing the predictive value of MS using three different definitions. The meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. PubMed and Web of Science were searched to retrieve eligible longitudinal studies published before June 1, 2014. The methodological qualities of the included studies were assessed independently using the Newcastle–Ottawa Scale (NOS), a validated instrument in assessing the quality of observational and nonrandomized studies. The meta-analysis evaluated the predictive value of MS for future CV events, stroke, and all-cause mortality. The outcomes of interest were total CV events (fatal and nonfatal CV events, such as coronary events, heart failure, stroke, and myocardial infarction), stroke (fatal and nonfatal), and all-cause mortality.
Morning blood pressure surge had 3 different definitions: (1) sleep-trough surge: calculated as the morning BP (the mean BP during 2 hours after wake-up) minus the lowest night-time BP (1-hour average of 3 BP readings centered on the lowest nocturnal BP reading); (2) pre-waking surge: defined as the morning BP minus the pre-waking BP (2-hour average BP before wakeup); and (3) rising BP surge, defined as the BP on rising minus the last BP reading in the 30 minutes before rising. Only systolic BP, rather than diastolic BP, was used to calculate the MS. Relative risk (RR) was used as a common risk estimate across studies, and treated HRs as relative risk. A random effects model was used to obtain the pooled RR in the presence of significant heterogeneity, whereas a fixed effect model was used in the absence of heterogeneity. The RRs and CIs of comparable studies were illustrated with forest plots. The predictive role of pre-waking and sleep-trough MS in CV events were analyzed separately. A separate meta-analysis was performed for total CV events, stroke, and all-cause mortality. The pooled RRs for high MS versus low MS (including both pre-waking and sleep-trough MS) were calculated for each of the outcomes.
Initially, a total of 756 relevant publications were identified, which were narrowed to 12 original articles by excluding 231 duplicates and 513 unrelated articles. Three of those articles were then excluded because the populations in these studies overlapped with those of other studies. One article did not use one of the classic definitions of MS, so it was excluded. Another article was excluded because of the small sample size and lack of essential data for calculating the risk estimates.
The authors included in the meta-analysis 7 eligible longitudinal studies that evaluated morning surge and followed 14,133 patients with a mean follow-up period of 7.1 years. All studies were observational cohort studies. Hypertensive, diabetic, and general populations were included. The included subjects were from Denmark, Belgium, Russia, Italy, Poland, France, Israel, Japan, China, Uruguay, and Brazil. The mean age of the populations ranged from 49 years to 72 years. For subjects with higher pre-waking MS than those with lower pre-waking MS, the pooled relative risk (RR) of all-cause mortality, stroke, and total CV events were 1.20 (95% confidence interval [CI]: .85-1.70, P = .290; 4 studies), 1.20 (95% CI: .94-1.53, P = .146; 3 studies), and 1.24 (95% CI: .60-2.53, P = .562; 3 studies), respectively. For subjects with higher sleep-trough MS, the pooled RR of all-cause mortality was 1.29 (95% CI: 1.11-1.52, P = .001; 4 studies).
These results indicated that only sleep-trough MS was statistically significantly associated with a higher risk of all-cause mortality, and that a higher pre-waking MS was associated with a higher risk of stroke, although the difference was not significant. The risk of all-cause mortality in subjects with increased sleep-trough MS was significantly higher compared with that in patients with lower sleep-trough MS. However, the association between high pre-waking MS and the risk of all-cause mortality, stroke, or total CV events was statistically non-significant. No significant publication bias was observed.
The authors acknowledged these limitations. First, no unified cutoff value of MS is established, so they used the cutoff values provided in the original articles. Therefore, bias was inevitable because the cutoff values differed among the articles. Second, the adjusted factors differed in each study, so the pooled RR of all the included studies provided less clear results. Third, they treated rising MS as pre-waking MS, which possibly resulted in increased heterogeneity. Fourth, their meta-analysis lacked robustness to explain possible heterogeneity among the original studies because of the limited number of related studies in the literature.
The authors concluded that excess sleep-trough morning blood pressure surge is a strong predictor for future all-cause mortality. Individuals with higher pre-waking morning blood pressure surge showed a tendency for increased risk of CV outcomes, but the differences were statistically insignificant. Morning blood pressure surge has the potential to find undetected hypertension.
4. Medicare Evidence Development & Coverage Advisory Committee (MEDCAC)
A MEDCAC was not convened for this reconsideration.
5. Evidence-Based Guidelines
The pertinent evidence-based guidelines are summarized below.
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018 May 15;71 (19):e127-e248
In 2017, a multi-society task force released the Guideline for Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. These Guidelines updated the 2003 JNC 7 (Chobanian et al., 2003) definition of hypertension. The Guidelines also moved the threshold for BP- lowering medication from SBP 140 mm Hg or DBP 90 mm Hg or patients with clinical CVD to 130 mm Hg or higher SBP or DBP of 80 mm Hg or higher. The Guidelines recommended initiating medical BP-lowering treatment for primary prevention in adults with an estimated 10-year atherosclerotic CVD risk of 10% or higher and an average SBP 130 mm Hg or higher or an average DBP 80 mm Hg or higher. The latter recommendation was based on the results of the SPRINT study, which demonstrated among nondiabetic patients at high risk for cardiovascular events, targeting a systolic blood pressure of less than 120 mm Hg, as compared with less than 140 mm Hg, resulted in lower rates of fatal and nonfatal major cardiovascular events and death from any cause (Whelton et al., 2015) and a number of meta-analyses of BP-lowering trials published since the JNC 7 Guidelines. The 2017 Guidelines also had seven recommendation for the use of ABPM, which also included recommendations for home BP monitoring (HBPM) (Table 10). .
| Table 11 |
|---|
ACC/AHA Guideline Recommendations on Out-of-clinic BP Monitoring
| COR |
LOE |
Recommendation |
| IIa [moderate recommendation] |
B-NR
[moderate quality, nonrandomized evidence] |
In adults with an untreated SBP greater than 130 mm Hg but less than 160 mm Hg or DBP greater than 80 mm Hg but less than 100 mm Hg, it is reasonable to screen for the presence of white coat hypertension by using daytime ABPM or HBPM before diagnosis of hypertension. |
| IIa [moderate recommendation] |
C-LD [limited data] |
In adults with white coat hypertension*, periodic monitoring with either ABPM or HBPM is reasonable to detect transition to sustained hypertension. |
| IIa [moderate recommendation] |
C-LD [limited data] |
In adults being treated for hypertension with office BP readings not at goal and HBPM readings suggestive of a significant white coat effect, confirmation by ABPM can be useful. |
| IIa [moderate recommendation] |
B-NR
[moderate quality, nonrandomized evidence |
In adults with untreated office BPs that are consistently between 120 mm Hg and 129 mm Hg for SBP or between 75 mm Hg and 79 mm Hg for DBP, screening for masked hypertension with ABPM or HBPM is reasonable. |
| IIb [weak recommendation] |
C-LD [limited evidence] |
In adults on multiple-drug therapies for hypertension and office BPs within 10 mm Hg above goal, it may be reasonable to screen for white coat effect with HBPM or ABPM |
| IIb [weak recommendation] |
C-EO
[consensus expert opinion] |
It may be reasonable to screen for masked uncontrolled hypertension with HBPM in adults being treated for hypertension and office readings at goal, in the presence of target organ damage or increased overall CVD risk. |
| IIb [weak recommendation] |
C-EO
[consensus expert opinion] |
In adults being treated for hypertension with elevated HBPM readings suggestive of masked uncontrolled hypertension, confirmation of the diagnosis by ABPM might be reasonable before intensification of antihypertensive drug treatment |
| COR: Class of recommendation
LOE: Level of evidence
*Among those not taking antihypertensive medication. |
Figures below excerpted from Whelton et al. 2017.
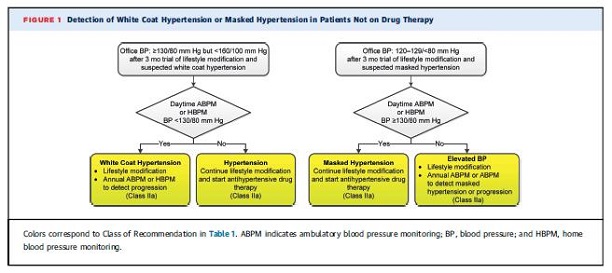
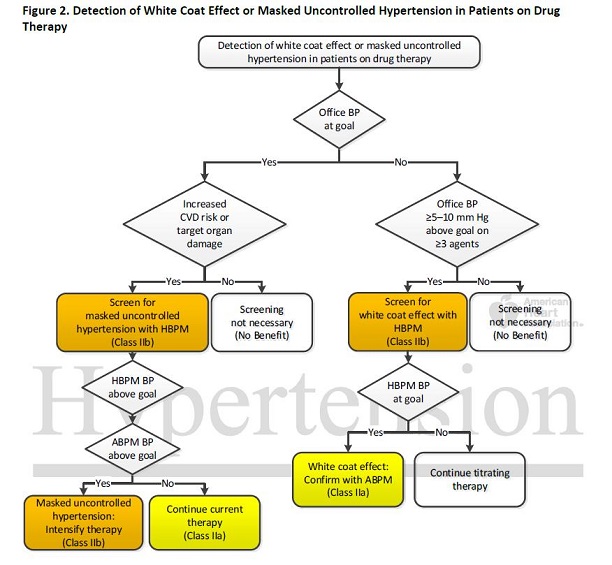
Whelton et al., 2017.
The figures above indicate that ABPM should be used with recommendations for diet, exercise and in combination with other BP from patient self-monitoring of their BP.
The guidelines also provide a guide to taking accurate OBPM:
| Table 12 Accurate measurement of BP |
|---|
| Key Steps for Proper BP Measurements |
Specific Instructions |
|---|
| Step 1: Properly prepare the patient |
1. Have the patient relax, sitting in a chair (feet on floor, back supported) for >5 min.
2. The patient should avoid caffeine, exercise, and smoking for at least 30 min before measurement.
3. Ensure patient has emptied his/her bladder.
4. Neither the patient nor the observer should talk during the rest period or during the measurement.
5. Remove all clothing covering the location of cuff placement.
6. Measurements made while the patient is sitting or lying on an examining table do not fulfill these criteria. |
| Step 2: Use proper technique for BP measurements |
1. Use a BP measurement device that has been validated, and ensure that the device is calibrated periodically.*
2. Support the patient’s arm (e.g., resting on a desk).
3. Position the middle of the cuff on the patient’s upper arm at the level of the right atrium (the midpoint of the sternum).
4. Use the correct cuff size, such that the bladder encircles 80% of the arm, and note if a larger- or smaller-than-normal cuff size is used (Table 9).
5. Either the stethoscope diaphragm or bell may be used for auscultatory readings (5, 6). |
| Step 3: Take the proper measurements needed for diagnosis and treatment of elevated BP/hypertension |
1. At the first visit, record BP in both arms. Use the arm that gives the higher reading for subsequent readings.
2. Separate repeated measurements by 1–2 min.
3. For auscultatory determinations, use a palpated estimate of radial pulse obliteration pressure to estimate SBP. Inflate the cuff 20–30 mm Hg above this level for an auscultatory determination of the BP level.
4. For auscultatory readings, deflate the cuff pressure 2 mm Hg per second, and listen for Korotkoff sounds. |
| Step 4: Properly document accurate BP readings |
1. Record SBP and DBP. If using the auscultatory technique, record SBP and DBP as onset of the first Korotkoff sound and disappearance of all Korotkoff sounds, respectively, using the nearest even number.
2. Note the time of most recent BP medication taken before measurements. |
| Step 5: Average the readings |
Use an average of ≥2 readings obtained on ≥2 occasions to estimate the individual’s level of BP. |
| Step 6: Provide BP readings to patient |
Provide patients the SBP/DBP readings both verbally and in writing. |
Because there were no randomized controlled trials of ABPM, these recommendations were based on the available observational research, much of it conducted outside of the US, that suggested that cardiovascular events and death are related to elevated ABPM, white coat hypertension, and masked hypertension, all which can only be measured with ABPM.
The authors concluded that ABPM provides enhanced ability to both diagnose hypertension and monitor treatment. They acknowledged that evidence is sufficient to recommend incorporating this tool into clinical practice, more knowledge about it is required. They recommended additional research on the relationship between ABPM and home BP measurement, the reproducibility of ABPM, and the inclusion of a broader range of ethnicities in research. Finally, they recommended trials with entry criteria and treatment goals based on BP measurements taken out of the office, including studies of masked and white coat hypertension.
US Preventive Services Task Force. Final Recommendation Statement High Blood Pressure in Adults: Screening. 2015
The USPSTF concluded with high certainty that the net benefit of screening for high blood pressure in adults is substantial. However, the evidence did not address the diagnostic accuracy of different blood pressure measurement protocols or identify a reference standard for measurement confirmation. For the current recommendation, the USPSTF examined the diagnostic accuracy of office blood pressure measurement, ambulatory blood pressure monitoring (ABPM), and home blood pressure monitoring (HBPM). The USPSTF also assessed the accuracy of these blood pressure measurements and methods in confirming the diagnosis of hypertension. In addition, it reviewed data on optimal screening intervals for diagnosing hypertension in adults. The USPSTF recommends that, in addition to office blood pressure measurement, ABPM and out of office BP monitoring may be used to confirm a diagnosis of hypertension after initial screening.
Parati G, Stergiou G, O'Brien E, et al.; European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability.. European Society of Hypertension practice guidelines for ambulatory blood pressure monitoring. J Hypertens. 2014 Jul;32(7):1359-66.
The authors reported the consensus of the European Society of Hypertension that ABPM should be provided to patients who will benefit from improved management of hypertension. The Society advised that ABPM be used in the following circumstances (albeit with higher BP thresholds than currently recommended):
- Identifying white-coat hypertension phenomena including:
- WCH hypertension in untreated individuals
- White-coat effect in treated or untreated individuals
- False resistant hypertension due to white-coat effect in treated individuals
- Identifying masked hypertension phenomena:
- Masked hypertension in untreated individuals
- Masked uncontrolled hypertension in treated individuals
- Identifying abnormal 24-h BP patterns
- Daytime hypertension
- Siesta dipping/post-prandial hypotension
- Nocturnal hypertension
- Dipping status/isolated nocturnal hypertension
- Assessing treatment
- 24-h BP control
- True resistant hypertension
The European Society of Hypertension also has recommendations for when to repeat ABPM:
- Indications for ABPM repetition to evaluate 24-h BP control:
- Severe or apparently resistant hypertension
- Presence of target organ damage
- Existence of comorbidities (e.g. diabetes)
- Positive family history of premature cardiovascular disease
- Indications for ABPM repetition at short time intervals (3–6 months or less):
- To confirm the diagnosis of white-coat or masked hypertension
- Confirmation of nocturnal hypertension
- Follow-up of high risk patients when optimal treatment is sought
- In cases of mild hypertension and low cardiovascular risk, ABPM may be repeated at 1- or 2-year intervals, while regular implementation of HBPM may better suit the needs of long-term follow-up.
O'Brien E, Parati G, Stergiou G, et al. European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension Position Paper on Ambulatory Blood Pressure Monitoring. J Hypertens. 2013 Sep;31(9):1731-68.
The authors reported an expansive guideline that provided information and evidence based recommendations on the ABPM device and software, indications for ABPM, and implementation of ABPM in clinical practice, among other topics.
Characteristics of ABPM devices
The guideline suggested that the validation of automated BP-measuring devices should be complemented by an overall quality check. It described the PA.NET International Quality Certification Protocol, which comprises quality criteria for BP-measuring devices that fulfilled basic validation criteria. Validations for devices by manufacturer name are available at the dabl® Educational Trust website (http://www.dableducational.org/). The guideline suggested that devices should be validated for the intended population. ABPM devices should be validated for use in the elderly, patients with kidney disease, pregnant women, obese patients, and children.
The guideline provided the following ABPM software recommendations:
Clinical report
- Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type
- Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated
- Average SBP, DBP, and heart rate to be displayed
- Nocturnal blood pressure decline (%) for SBP and DBP
- Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-hour period, daytime and night-time, with standard deviations and number of valid blood pressure readings
- Facility for showing error readings, if required
Optional requirements
- Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are fulfilled
- Facility to plot heart rate and mean blood pressure
- Trend report for comparing repeated ambulatory blood pressure measurement recordings
- Ability to centrally host data
The guidelines provided helpful recommendations for using ABPM in the clinical setting and advised that ABPM results must be interpreted under medical supervision.
Basic requirements
- Patients must be capable of understanding and coping with the device
- Ambulatory blood pressure measurement should be performed preferably on a routine working day
- Repeat ambulatory blood pressure measurements should be on similar days
- 10–15 min needed to program and fit the device, depending on first or follow-up recording
- Patient should be relaxed in quiet room Advice to the patient
- Procedure should be explained
- Patients should be told to follow their usual daily activities but to remain still during measurement with the arm relaxed at heart level
- Instruct patient to place monitor on the bed or beneath the pillow at night
- Warn patient not to take a shower or bath
- Advise patient against driving, but if necessary, stop driving if possible during measurement
- Mark the brachial artery so that if the cuff becomes loose, the patient can refit it
- Give patient oral and written instructions and a diary card to record the time of drug intake, the time of rising and going to bed, and any symptoms
- Instruct patient how to switch off the monitor in case of malfunctioning, such as repeated inflation
- Instruct patient on how to remove and inactivate monitor after 24 hour
Pediatric guidelines
Flynn JT, Kaelber DC, Baker-Smith CM, et al; Subcommittee on Screening and Management of High Blood Pressure In Children. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics. 2017; 140(3):e20171904.
These pediatric hypertension guidelines were issued to align with the 2017 Guidelines (Whelton et al., 2017). The guidelines recommended the following:
- Taking BP in children annually and at every encounter with children with certain risk factors such as obesity, renal disease, diabetes, and coarctation.
- ABPM should be performed for confirmation of hypertension in children and adolescents with office BP measurements in the elevated BP category for 1 year or more or with stage 1 HTN over 3 clinic visits (BP norms vary with the size of the child
- Routine ABPM should be strongly considered in children and adolescents with high-risk conditions to assess HTN severity and determine if abnormal circadian BP patterns are present, which may indicate increased risk for target organ damage.
- Children and adolescents with suspected WCH should undergo ABPM.
- Children and adolescents with suspected WCH should undergo ABPM.
- Home BP monitoring should not be used to diagnose HTN, MH, or WCH but may be a useful adjunct to office and ambulatory BP measurement after HTN has been diagnosed.
Device validation protocol guideline
Stergiou G, Alpert B, Mieke S, et al. A Universal Standard for the Validation of Blood Pressure Measuring Devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. J Hypertens. 2018;36:472‐478.
The authors reported on nine key aspects of an optimal clinical validation procedure to assess the accuracy of blood pressure (BP) measuring devices. These methodological and clinical aspects were agreed on by the US Association for the Advancement of Medical Instrumentation (AAMI), the European Society of Hypertension (ESH), and the International Organization for Standardization (ISO) representatives which would form the basis for developing a single universal standardized protocol for the validation of BP monitors and establish minimum standards of device accuracy and performance. Global consensus was based on the evidence from previous validation studies using the AAMI, British Hypertension Society (BHS), ESH-International Protocol (ESH-IP) and ISO protocols, new statistical analyses of study and subgroup sample sizes and power calculations, and expert opinion. This preliminary document does not present a detailed description of all the aspects of the validation procedure, which will become available as the organizations involved develop the universal protocol in more detail.
- For the validation study efficacy measure, a device was considered acceptable if the estimated probability of tolerable error (<10 mm Hg) was at least 85%, based upon an average of three BP readings compared to a reference BP measurement method.
- The validation study sample size of at least 85 subjects are required for an AAMI/ISO/ESH validation study.
- For multiple cuff-size stratified subgroup analyses:
- The minimum number of subjects to be tested per cuff size was determined and depends on the number of the different test device cuffs available. Cuff subgroup sample sizes were not intended for use in separate analyses for each cuff size, but were intended to ensure an even representation of all cuff sizes with a minimum number of participants.
- Requirements were set for the percentile distribution of participants categorized by their arm circumference according to the specified range of use of the test device.
- Special population studies with smaller sample sizes should be performed only after a full general population study has been successfully completed. If the device is intended only for a special population, then a full 85-subject study is required. General population and special population studies were defined as follows:
- A general population study should include only subjects older than 12 years.
- Special populations are regarded as follows and can include at least: (i) age <3 years, (ii) pregnancy including pre-eclampsia, (iii) arm circumference >42 cm, or (iv) atrial fibrillation. Other special populations may be added as special groups.
- Special population studies to include ≥35 subjects, provided that a separate general population study of n = 85 has been completed successfully. For special populations, BP distribution criteria should be different from those of general population studies. Data should be analyzed independently of general population study data.
- Studies in pregnancy to include 45 women of whom 15 have pre-eclampsia, 15 with gestational hypertension, and 15 normotensive. Korotkoff K5 shall be used for reference diastolic BP.
- For devices intended for adults and children, 35 subjects aged 3-12 years can be included and analyzed together with 50 subjects aged >12 years. Mean BP difference and standard deviation (SD) shall also be reported separately for age 3-12 and >12 years age groups. Korotkoff K5 shall be used for reference diastolic BP.
- For BP data collection method:
- The same arm sequential BP measurement is the preferred method for validation.
- The same arm simultaneous method was eliminated.
- For reference BP measurement and validation procedure, the auscultation standard is retained for reference BP measurement with measurements taken simultaneously by two trained observers blinded to each-other’s readings and to the measurements taken with the test device.
- Reference BP measurement to be performed with mercury sphygmomanometers or accurate non-mercury devices. The accuracy of non-mercury devices shall be evaluated at the beginning of each study.
- Detailed description of cuffs used for reference BP measurement shall be provided.
- The test device cuffs shall not be used for reference BP determination.
- For validation criteria and reporting,
- The mean BP difference (test versus reference) and its standard deviation (SD), i.e., Criteria 1 and 2 of the ANSI/AAMI/ISO 81060-2 (Non-invasive sphygmomanometers - Part 2: Clinical investigation of automated measurement type. American National Standards Institute; 2013. ANSI/AAMI/ISO 81060-2, http://webstore.ansi.org) will be applied in the AAMI/ESH/ISO validation data evaluation. The same criteria used for systolic and diastolic BP measurements.
- The number of absolute BP differences within 5, 10, and 15 mm Hg, and the standardized Bland-Altman scatterplots will be presented.
- For validation of other BP monitors,
- Separate validation protocols will be developed for continuous, cuffless and central BP monitors.
- For quality and reliability of validation study reports,
- Tools need to be developed to prevent protocol violations and incomplete reporting, and to secure appropriate and transparent patient and data selection.
- Detailed forms should be developed to fill in all the data from validation studies that need to be reported.
6. Professional Society Recommendations / Consensus Statements / Other Expert Opinion
An internet search located a number of professional society position statements exclusively concerning ABPM. These are reviewed in Section 5.
The requestors, the American Heart Association and the American Medical Association, submitted a professional society position statement by way of their letter requesting a reconsideration of the NCD, which may be found on our website.
Additional professional society recommendations, consensus statements and other expert opinions included those submitting comments during the public comment period. They include, but are not limited to: Cleveland Clinic, Stanford University School of Medicine, Washington University School of Medicine, Heart Rhythm Society and other institutions and individuals.
7. Public Comment
Public comments sometimes cite the published clinical evidence and give CMS useful information. Public comments that give information on unpublished evidence such as the results of individual practitioners or patients are less rigorous and therefore less useful for making a coverage determination.
CMS uses the initial public comments to inform its proposed decision. CMS responds in detail to the public comments on a proposed decision when issuing the final decision memorandum. All comments that were submitted without personal health information may be viewed in their entirety by using the following link: https://www.cms.gov/medicare-coverage-database/details/nca-view-public-comments.aspx?NCAId=294
Initial Comment Period: October 9, 2018 – November 8, 2018
During the initial 30-day comment period, CMS received 103 comments from hospitals, internists, cardiologists, nephrologists, pediatricians, physician groups and other healthcare professionals. One hundred two comments were in favor of expanding coverage of ABPM, many of which referenced the USPFTF recommendation. Certain comments state that new ABPM recommendations have been adopted in medical practice. One comment was off topic.
Second Comment Period: April 19, 2019 through May 19, 2019
During the comment period following release of the proposed decision memorandum, CMS received 63 comments, one of which was omitted from publication on the CMS website due to extensive personal health information. All except for one comment expressed support for our proposed decision to expand coverage with certain caveats discussed below.
The majority of comments were from individual physicians and those representing hospitals and universities, along with other health professionals.
There were comments on behalf of professional societies and patient advocacy groups including the requestor, the American Heart Association. Those organizations offering remarks include National Association of Chronic Disease Directors, American Society of Pediatric Nephrology, American College of Cardiology, Advocate Aurora Health, American College of Medical Quality, National Association of Community Health Centers, Preventive Cardiovascular Nurses Association, Connected Health Initiative and Pediatric Diagnostics. The New York City Department of Health and Mental Hygiene, Hill Rom, Medtronic and Kaiser Permanente also submitted comments in favor of expanded coverage with caveats. CMS appreciates all submitted comments.
Device Validation Protocol
Comment: Twenty comments recommended that a specific blood pressure device validation protocol be used rather than directing readers to a specific website that summarizes whether a device has undergone validation.
Response: CMS appreciates this comment and removed the dabl device validation website from the final decision memorandum because the evidence indicated there was no scientific oversight of this registry and there are currently no validation registries the US. Note that the expanded evidence section addresses the publications by Cohen, et al. (2019) and Stergiou, et al. (2018) on validation protocols.
Lifestyle Intervention
Comment: Twenty-two comments recommended that CMS remove the requirement for three months of lifestyle interventions prior to ABPM use, as this is not consistent with the 2017 American Heart Association/American College of Cardiology Guidelines for Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults, nor those of the United States Preventive Services Task Force.
Response: We appreciate the comment and have revised based on the evidence and guidelines. We emphasize as did the professional society guidelines the importance of lifestyle interventions and recommend physicians and patients follow separate professional recommendations on risk factor reduction. The three month requirement has been removed from the final decision.
Blood pressure code ranges
Comment: Twelve comments addressed item (2) in the final decision language. They believe the document should read, "between 120 mm Hg and 129 mm Hg for systolic pressure or between 75 mm Hg and 79 mm Hg for diastolic blood pressure".
Response: CMS appreciates this comment and we have revised the final decision memorandum to reflect the 2017 professional society Guidelines.
Management aspect of coverage
Comment: CMS received 14 comments requesting clarification on the "management" aspect of the proposed decision, given that the request focused on diagnosis only. They also note that clinical guidelines for management of hypertension differs from the guidelines for diagnosis.
Response: CMS appreciates this comment and we have removed the word management.
Pediatric beneficiaries
Comment: Twelve comments recommended that CMS include pediatric patients in the final decision memorandum so as to recognize their unique needs, as well as the American Academy of Pediatrics guidelines.
Response: CMS appreciates this comment. We note that pediatric Medicare beneficiaries are those with end stage renal disease. These would potentially be covered for ABPM. Of 70 references received, two concerned pediatric hypertension. The expanded evidence section of the final decision memorandum contains a section addressing the publications by Flynn, et al. (2017) and Iturzaeta, et al. (2018) on hypertension in pediatric populations. The American Academy of Pediatrics hypertension guidelines were issued to align with the 2017 Guidelines (Whelton, et al.). Masked hypertension and white coat hypertension are important predictors of adverse cardiovascular disease outcomes.
Nocturnal hypertension
Comment: Seventeen comments suggested that CMS address nocturnal hypertension in the final decision memorandum.
Response: The expanded evidence section addresses the publication by Hermida, et al. (2018) and the benefit of measuring nighttime blood pressure for beneficiaries that may have undetected hypertension, such as suspected nocturnal hypertension, which is related to an increased risk of cardiovascular disease. The measurement of nocturnal hypertension is implicit in 24-hour ABPM studies. The use of ABPM as covered by this NCD will allow detection of nocturnal hypertension.
White coat hypertension in treated versus untreated patients
Comment: Some commenters questioned whether ABPM services would be covered for both patients with undiagnosed hypertension and patients already diagnosed with hypertension (white coat effect versus white coat hypertension).
Response: Because some of the reviewed evidence grouped WCE with WCH, we could not determine the separate impacts of the two conditions. Based on this, we removed the word ‘untreated’ from our previous NCD. Under this NCD, we consider WCE WCH together.
Average Office Blood Pressure
Comment: Sixteen comments include recommendations for accurate determination of office blood pressure. It is pointed out the 2007 AHA/ACC guidelines state that "an average of ≥2 readings be obtained on ≥2 occasions [be used] to estimate the individual level of office blood pressure."
Response: We agree. For beneficiaries with suspected white coat hypertension or suspected masked hypertension, two separate clinic/office visits with the average from at least two separate measurements be made at each visit. In this way, a more accurate estimate can be obtained.
Out-of-office measurement
Comment: Eighteen comments stated that references to blood pressure measurement taken outside of the office be removed from the final decision memorandum. Their rationale is that this may be construed to mean home blood pressure monitoring be used first prior to ABPM. They state that the USPSTF recommended means for detecting high blood pressure is using ABPM as the out-of-office method, unless, when not available, home BP measurement "may be acceptable". Home blood pressure monitoring (i.e., out-of-office), is not a covered service and is therefore not reimbursed. Buying a monitor and using it appropriately places a burden on the beneficiary. They recommend that requiring out-of-office home BP monitoring prior to ABPM should be deleted.
Response: We appreciate the comment and note that the 2017 ACC/AHA guidelines (Whelton, 2017) recommend the use of out of office blood pressure measurements with a Class of Recommendation grade I (recommendation 4.2). Based on the evidence, we are maintaining this criterion.
Coding and payment
Comment: Two commenters requested that the final decision memorandum contain coding and payment information for ABPM.
Response: CMS appreciates these comments. Coding and payment guidelines are outside of the scope of a national coverage determination as defined in section 1869(f)(1)(B) of the Social Security Act. CMS will address coding information at a later date.
Measurements only at night
Comment: One requestor suggested that ABPM be performed only at night.
Response: The AHA/ACC guidelines state that ABPM be performed for at least 24 hours.
Frequency of testing
Comment: CMS received one comment stating that ABPM be measured 6 times during the first year, then every 2 years.
Response: Under the NCD, for eligible patients, ABPM is covered once per year. Other indications for uses of ABPM may be made by local Medicare Administrative Contractor.
Self-measured blood pressure
Comment: One comment favored self-measured blood pressure as a practical alternative to ABPM.
Response: Guidelines by AHA/ACC do not include self-measured blood pressure.
VIII. CMS Analysis
National coverage determinations are determinations by the Secretary with respect to whether or not a particular item or service is covered nationally by Medicare (§1869(f)(1)(B) of the Act). In general, in order to be covered by Medicare, an item or service must fall within one or more benefit categories contained within Part A or Part B, and must not be otherwise excluded from coverage. Moreover, with limited exceptions, the expenses incurred for items or services must be reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member." (§1862(a)(1)(A) of the Act).
When making national coverage determinations, we evaluate the evidence related to our analytic questions based on the quality, strength and totality of evidence presented in the reviewed literature. As part of this evaluation, it is important to consider whether the evidence is relevant to the Medicare beneficiary population. In determining the generalizability of the results of the body of evidence to the Medicare population, we consider, at minimum, the age, race and gender of the study participants. There are a number of structured methods for evaluating diagnostic tests. In past diagnostic imaging NCDs, we considered the evidence in the hierarchical framework of Fryback and Thornbury (1991) where Level 1 concerns technical quality of the images; Level 2 addresses diagnostic accuracy, sensitivity, and specificity of the test; Level 3 focuses on whether the information produces change in the physician's diagnostic thinking; Level 4 concerns the effect on the patient management plan; Level 5 measures the effect of the diagnostic information on patient outcomes; and Level 6 examine societal costs and benefits of a diagnostic imaging technology. In our analysis, we generally look for sound evidence that shows the test is analytically and clinically valid (Levels 1-2) and that use of the test to guide treatment improves health outcomes (clinical utility, Levels 3-5).
In the case of ABPM, there is no randomized controlled trial demonstrating that use of ABPM significantly improves health outcomes such as all-cause mortality. However, there exists a strong body of evidence from population-based and large cohort studies that show diagnosis of hypertension changes clinical management (including use of medications) that in turn improves health outcomes including survival (recent publications include Ettehad et al., 2016, Law et al., 2009, Sundstrom et al., 2014). In our prior NCD and analysis (https://www.cms.gov/medicare-coverage-database/details/nca-details.aspx?NCAId=5), the ability of ABPM to diagnosis hypertension and clinical utility for certain patients were established.
For this reconsideration, the specific assessment questions for ABPM are:
- In patients with suspected white coat hypertension who are not on treatment for elevated blood pressure, does ABPM improve health outcomes?
- In patients with white coat hypertension, does ABPM improve health outcomes?
- In patients with suspected masked hypertension, does ABPM improve health outcomes?
Our analysis includes peer-reviewed, published clinical studies and guidelines pertaining to blood pressure measurement in the clinical office compared to ambulatory blood pressure monitoring and the phenomena and sequelae of overestimating and underestimating blood pressure monitoring in the office. We considered evidence of ABPM from one clinical trial of out of office blood pressure measurement on patient outcomes. The bulk of the evidence comes from European population-based studies that have used 24-hour ABPM to measure blood pressure while patients are living their normal lives, and followed these patients to measure outcomes as they relate to ABPM and OBPM. We believe these studies are relevant to the Medicare population since hypertension is a ubiquitous health condition across the globe and acknowledged as the number one cause of death worldwide and in the US (Lim et al., 2012, Forouzanfar, et al., 2017, CDC, 2017, Danaei et al., 2009, Lewington et al., 2002).
Medicare’s coverage of ABPM is restricted to patients with documented WCH who have no evidence of target organ damage. As a result of our present analysis, we now believe that ABPM has more benefit than only ruling out WCH. It is an essential tool in managing hypertension to reduced mortality and improve other health outcomes for Medicare beneficiaries. Our analysis also takes into account considerable evolution in the definition of high blood pressure and approaches to its treatment that have occurred since our 2001 ABPMNCD.
Question 1: In patients with suspected white coat hypertension who are not on treatment for elevated blood pressure, does ABPM improve health outcomes?
Our answer to question 1 is yes. There are a number of structured methods for evaluating diagnostic tests. In past decisions on diagnostic imaging, we considered the evidence in the hierarchical framework of Fryback and Thornbury (1991) where Level 2 addresses diagnostic accuracy, sensitivity, and specificity of the test; Level 3 focuses on whether the information produces change in the physician's diagnostic thinking; Level 4 concerns the effect on the patient management plan and Level 5 measures the effect of the diagnostic information on patient outcomes. For diagnostic tests, we have focused on evidence on clinical utility, i.e., use of the test improves health outcomes (equivalent to Level 5 above). For diagnosis of hypertension by ABPM, the evidence supports the conclusion that use of ABPM improves BP control and treatment, which in turn will lead to decreased target organ damage, and improved health outcomes including survival as established by numerous population-based studies. Use of ABPM could also decrease overtreatment resulting from false positives (white coat hypertension). While there has been no high-quality randomized controlled clinical trial to evaluate the direct effects of ABPM on physician decision making and patient outcomes, one trial of out-of-office BP measurement suggested that patient knowledge of hypertension may have a positive effect on long term outcomes (Kaczorowski et al., 2011, Dahrouge et al., 2018). Through the established chain of evidence that currently exists as described in our prior decision (2003), we believe a more accurate diagnosis of hypertension will directly guide physician treatment and improve patient health outcomes.
Although more than 75% of adults aged >65 years have BP of >130/80, hypertension should be confirmed by ABPM before treatment (Whelton et al., 2017). Out-of-office measurement of BP is recommended by both the USPSTF (before treatment for hypertension) and the most recent blood pressure detection guidelines (Sui, 2015, Whelton et al., 201). While the most recent guidelines have recommendations for taking BP in the clinical office that include having the patient avoid caffeine, using a calibrated device taking 2 measurements, using both arms, (Whelton et al, 2017), we recognize this may pose a barrier at busy practices, and that ABPM remains a recommended diagnostic tool for certain patients.
As discussed in the introduction, recent guidelines lowered the threshold for the definition and treatment of BP. This new definition effectively increases the population prevalence of hypertension (based on reported antihypertensive medication use) from 64% and 63% of men and women ages 64- 74 years, respectively, to 77% and 75%; and from 71% and 78% in men and women ages 75 years and older, respectively, to 79% and 85% (Whelton et al., 2017). More people will benefit from ABPM.
Evidence incorporated in the 2014 meta-analysis conducted by the USPSTF indicates that elevated BP as measured by ABPM is a better predictor of long term cardiovascular outcomes than OBPM, which has relatively low sensitivity and moderate PPV (Piper, et al., 2014). Banegas et al. (2017) found that misclassification of hypertension status by OBPM was over 40%. Thus, ABPM fulfills Fryback and Thornbury’s (1991) Level 2, ABPM is a more accurate method of measuring BP than OBPM. Piper at al. (2014) also reported increasing 24-hour systolic ABPM, independent of OPBM, was consistently associated with increased risk for fatal and nonfatal stroke events. The authors concluded that ABPM should be considered the reference standard for evaluating BP. Their results also indicated that OBPM frequently misdiagnoses patients by overestimating BP, which could lead to overtreatment. Overtreatment can result in hypotension, syncope, bradycardia, electrolyte abnormalities, falls, and acute kidney injury (SPRINT Research Group, 2015).
Several researchers have reported that a substantial number of patients, both untreated and treated for hypertension, whose OBPM is elevated are normotensive when tested at home with ABPM or other methods (white coat hypertension). One study reported that WCH occurred in more than 40% of untreated patients and in nearly 35% of treated patients (Benegas et al., 2015, Banegas et al., 2017). The most recent study by Banegas et al. (2018) found that elevated ABPM was related to both all- cause mortality and cardiovascular mortality. All of these data are from a Spanish population. There are no comparable in-depth US studies which limits the relevance of the findings to the Medicare population. However, the relationship between hypertension and morbidity and mortality has been underscored in numerous analyses of data from US and global populations (Lim et al., 2012, Forouzanfar, et al., 2017, CDC, 2017, Danaei et al., 2009, Lewington et al., 2002). As supported by the AHA and professional societies, we believe the world data on hypertension and treatment are relevant and generalizable to the US population.
In a nested case control study derived from an international cohort, in which the prevalence of WCH was 11.3% (all ages), the authors found that in patients with WCH, adverse outcomes were restricted to older (over age 60 yrs.) high risk patients. Low risk patients had the same long term outcomes as normotensives. This study suggests that physicians should carefully evaluate their Medicare-aged patients for the presence of WCH. In the US, the results from the Dallas Heart Study also indicated that WCH is associated with cardiovascular events. Prevalence of WCH was only 3% in this study. However, this study could not measure the true prevalence of WCH in the US, because office and out of office BP were measured by trained research staff and ABPM were not done.
Question 2: In patients with white coat hypertension, does ABPM improve health outcomes?
Our answer to question 2 is yes. Cuspidi et al. (2018) followed a population-based cohort to evaluate whether patients with WCH at baseline developed metabolic syndrome (defined by clustering of multiple risk factors, such as high-normal or elevated BP, hyperglycemia, low high-density cholesterol, elevated triglycerides and abdominal obesity. The authors found a doubling of risk of incident metabolic syndrome in the WCH patients, suggesting that these patients should be monitored. Mancia et al. (2015) found that patients with WCH during more than one (compared with WCH on 1 of 2 visits) had a greater risk of cardiovascular mortality and all-cause mortality, suggesting that physicians should determine whether there is consistent or transient WCH. Franklin el al. (2016), Mancia et al. (2015), and Tientcheu et al. (2015) reported that patients with WCH are also more likely to other risk factors for adverse cardiovascular outcomes.
Banegas, et al., followed a population of nearly 65,000 people (aged 18 years and older) finding that treated and untreated patients with WCH advanced to adverse outcomes more than 9 times more quickly than did normotensives. Huang et al. (2017) combined 14 observational studies of more than 30,000 people in a meta-analysis. The findings indicated that untreated WCH patients, compared with normotensives, had a significantly increased of adverse outcomes and that this was not true of treated patients with WCH.
The evidence strongly suggests that WCH patients have a different trajectory to cardiovascular disease and other sequelae than do normotensive patients. Use of ABPM has utility for patients with white coat hypertension.
Question 3: In patients with suspected masked hypertension, does ABPM improve health outcomes?
Our answer to question 3 is yes. Masked hypertension occurs when OBPM is normal but ABPM is elevated. Wang, et al., (2017) estimated that the prevalence of masked hypertension in US adults with the pre-2017 definition of normotension and not taking antihypertensive medication is 6.6% in patients with OBPM <120/80 mm Hg, 17.3% in patients with OBPM 120/80-<130/85, and 29.7% in patients with OBPM >130/85 mm Hg. Masked hypertension is more prevalent in males (18.1% in men vs. 7% in women), in people aged 65 years and older (28%) and in non-Hispanic whites and blacks (12.4% and 15.7%, respectively).
Masked hypertension is a major risk factor for adverse outcomes. Banegas et al. (2018) found hazard ratios of 2.83 for all-cause mortality and 2.85 for cardiovascular mortality among patients with masked hypertension in both treated and untreated patients. The same analysis indicated patients with masked hypertension progressed to all-cause mortality more than 20 years earlier than normotensives. Cuspidi et al. (2018) found a similarly high association between masked hypertension and incident metabolic syndrome. The meta-analysis by Palla et al. (2018), which combined population based cohort studies to achieve a sample size of 14,729 patients found that composite cardiovascular events occurred in 12.3% of untreated patients with masked HTN compared and 5.1% of patients with normotension (OR 2.91, 95% CI 2.54–3.33) and in 27.9% of treated patients with masked hypertension compared with 15.5% of treated patients with normotension (OR 2.03, 95% CI 1.52–2.72).
These data, all from population based cohort studies, suggest that masked hypertension may occur in patients with both untreated and treated for hypertension and that the elderly are at particularly high risk of having undetected hypertension. Use of ABPM has utility for patients with masked hypertension.
Other considerations
Nocturnal hypertension
The evidence suggests that patients with nighttime BP measurements, also called asleep blood pressure, that fulfill the diagnosis of suspected nocturnal hypertension, a nondipping or reduced or absence of dipping blood pressure phenotype (Hermida, 2018), and exaggerated morning BP surge (Xie, 2015) are associated with an increased risk for adverse cardiovascular disease outcomes. We acknowledge that measurement of nighttime BP, dipping status, and morning blood pressure surge has utility for Medicare beneficiaries having undetected hypertension, e.g., nighttime BP for suspected nocturnal hypertension. These ABPM parameters are implicit in 24 hour ambulatory blood pressure monitoring and so these BP indices can be derived from 24 hour ABPM recordings.
Pediatric hypertension
The evidence suggests that masked hypertension (Iturzaeta, 2018) and white coat hypertension may occur among children with risk factors. The 2017 pediatric hypertension guidelines (Flynn et al., 2017) were issued to be in parallel with the 2017 adult hypertension guidelines (Whelton, et al., 2018). Our decision provides coverage or ambulatory blood pressure monitoring for the diagnosis of hypertension in children if they are eligible for Medicare. We acknowledge that children under the age of 20 years only qualify for Medicare if they have end-stage renal disease (ESRD). Children over the age of 20 years qualify for Medicare after receiving Social Security Disability Insurance (SSDI) benefits for at least two years (24 months) or have end-stage renal disease.
Device validation protocol
In an article submitted by a public commenter, a review by Cohen, et al., (2019) states that there is no validation requirement for marketing a BP device in the US and that publicly available information on validation status of widely used BP devices is limited. The authors report that in the past, device validation listings were established to provide consumers, healthcare providers, academic researchers, and industry public access to information summarizing which devices have been validated and which criteria were used. CMS agrees with the public comment about the limitations of the Dabl Educational Trust. A limitation of the Dabl registry is the classification of devices validated using the Association for the Advancement of Medical Instrumentation (AAMI)/American National Standards Institute (ANSI)/International Organization for Standardization (ISO) protocol is listed as "not recommended", citing questionable evidence for this lack of validation. There is no longer any clear scientific oversight or regular updating of the Dabl registry (Cohen, 2019).
Professional hypertension societies have sections of their websites dedicated to Validated Device Listings (VDLs) of devices available for purchase in their respective countries. Examples include Hypertension Canada, the British and Irish Hypertension Society, and the Japanese Society of Hypertension (Cohen, 2019). As an example, the Hypertension Canada device listing (https://hypertension.ca/hypertension-and-you/managing-hypertension/measuring-blood-pressure/devices/) requires a manufacturer application and published validation data. It divides devices into those validated using the British Hypertension Society or AAMI/ANSI/ISO protocol (Gold tier) and European Society of Hypertension International Protocol18 (Silver tier) (Cohen, 2019).
Cohen, et al., (2019) reported that many devices are sold on the market without rigorous evaluation of the accuracy of the device. The authors stated that The American Medical Association (AMA) is leading a group of individuals and organizations in the field of hypertension and BP measurement to create and develop a transparent and easily accessible resource for identifying validated BP devices, the AMA Validated Device Listing (VDL) (https://www.ama-assn.org/delivering-care/hypertension/ama-aha-developing-list-validated-bp-monitors). The primary impetus for the AMA VDL was lack of any legal requirement in the United States for devices to undergo rigorous validation testing for clinical accuracy. There is no listing of devices available in the United States that have gone through validation testing for clinical accuracy. For a device to be listed in the AMA VDL, manufacturers will have to include in their application information on the validation protocol used in the validation study and a summary of the validation data either preferably, published in a peer-reviewed publication or from an independent third-party validation testing study conducted by a qualified entity, such as an academic institution or credible research entity with expertise in BP measurement and knowledge of validation protocols and validation study requirements (Cohen, 2019). As with other registries, the only assurance that validation protocols were performed correctly is by peer review. A major difference between the AMA VDL and the Hypertension Canada and British and Irish Hypertension Society device listings is the distinction of the validation protocols deemed acceptable. The proposed AMA VDL criteria were open for public comment during the summer of 2018. In the fall of 2018, the AMA convened with a panel of experts to address the public comments. The AMA VDL is currently undergoing administrative approvals and starting production; the AMA plans to make the VDL available for public use in early to mid-2019 (Cohen, 2019). CMS supports the AMA and the professional hypertension societies, such as Hypertension Canada, in their efforts to validate ambulatory blood pressure devices.
Accurate Blood Pressure Measurement
Accurate BP measurements are important to improve health outcomes. Table 12 above describes the method of BP measurement recommended by Whelton et al., 2017).
The guidelines also noted that "[f]urther research on improving accuracy of office BP measurements, including number of measurements, training of personnel measuring BP, and device comparisons, will help standardize care and thus improve outcomes."
Behavioral interventions
An important component of the treatment of hypertension and heart disease in general is behavior risk factor reduction also referred to as lifestyle modification. Medicare covers several behavioral intervention services for certain patients.(https://www.cms.gov/medicare-coverage-
database/details/ncd-details.aspx?NCDId=342&ncdver=2&NCAId=242), health diet interventions (https://www.cms.gov/medicare-coverage-database/details/ncd-details.aspx?NCDId=348&ncdver=1&NCAId=248) and physical activity (https://www.cms.gov/medicare-coverage-database/details/ncd-details.aspx?NCDId=353&ncdver=1&NCAId=253).
Health disparities
As described in the introduction, African Americans have the highest risk of hypertension (CDC, 2017). In the Multi-Ethnic Study of Atherosclerosis (MES), the percentage of the population developing hypertension over their lifetimes was higher for African Americans and Hispanics than for whites and Asians. For adults 45 years of age without hypertension, the 40-year risk of developing hypertension was 93% for African-American, 92% for Hispanic, 86% for white, and 84% for Chinese adults. The results from the NHANES survey also suggest that hypertension and uncontrolled hypertension may be more prevalent among lower income groups and in the very aged (CDC, 2017).
Nearly all of the studies of WCH have been European. The study by Wang et al. (2017), which found that masked hypertension was somewhat higher in non-Hispanic blacks than non-Hispanic whites (15.7% vs. 12.4%), was based on an employee sample and does not necessarily represent the Medicare population. The study by Tientcheu et al. (2015), which was based on the representative Dallas Heart Study found a higher prevalence of WCH, masked hypertension, and sustained hypertension among blacks. However, this study did not use ABPM and the BP measures were more precise than those done in usual clinic settings. Thus, this study did not represent the true prevalence of WCH and masked hypertension in the black population.
Although there are many gaps in the research on the use of ABPM in ethnic groups and in the estimates of prevalence of WCH and masked hypertension, it is a universal health concern that is not restricted to a particular subpopulation. It is particularly relevant among the aged population.
Randomized controlled trials of antihypertension therapy have shown it to be effective in reducing the risk of cardiovascular disease and mortality in multiple populations (Ettehad et al., 2016, Law et al., 2009, Sundstrom et al., 2014).
Summary
Based on our analysis of the peer-reviewed medical literature, we have determined that the evidence is sufficient for expansion of Medicare coverage of ABPM. Almost all public commenters agreed with the expansion of coverage. As such, we have modified our 2001 NCD.
First, we have removed the 2001 requirement that OBPM be measured at >140/90 on two separate occasions. The 2017 guidelines revised the threshold definition of hypertension (Whelton et al 2017) from a SBP >140/90 mm Hg to 130-139 or DBP 80-89 mm Hg.
Second, we have removed the 2001 requirement that there be no evidence of end-organ damage. We believe that the published evidence does not support this this criterion.
Third, there is a substantial proportion of patients who may appear to be in control or be normotensive, but have masked hypertension. The published evidence supports the use of ABPM to improve outcomes.
IX. Conclusion
-
The Centers for Medicare & Medicaid Services (CMS) has determined that the evidence is sufficient to cover ambulatory blood pressure monitoring (ABPM) for the diagnosis of hypertension in Medicare beneficiaries under the following circumstances:
- For beneficiaries with suspected white coat hypertension, which is defined as an average office blood pressure of systolic blood pressure greater than 130 mm Hg but less than 160 mm Hg or diastolic blood pressure greater than 80 mm Hg but less than 100 mm Hg on two separate clinic/office visits with at least two separate measurements made at each visit and with at least two blood pressure measurements taken outside the office which are <130/80 mm Hg.
- For beneficiaries with suspected masked hypertension, which is defined as average office blood pressure between 120 mm Hg and 129 mm Hg for systolic blood pressure or between 75 mm Hg and 79 mm Hg for diastolic blood pressure on two separate clinic/office visits with at least two separate measurements made at each visit and with at least two blood pressure measurements taken outside the office which are ≥130/80 mm Hg.
ABPM devices must be:
- capable of producing standardized plots of blood pressure measurements for 24 hours with daytime and night-time windows and normal blood pressure bands demarcated;
- provided to patients with oral and written instructions and a test run in the physician’s office must be performed; and
- interpreted by the treating physician or treating non-physician practitioner.
For eligible patients, ABPM is covered once per year.
- Coverage of other indications for ABPM are at the discretion of the Medicare Administrative Contractors.
See Appendix B for the manual language.
APPENDIX A
General Methodological Principles of Study Design
(Section VI of the Decision Memorandum)
When making national coverage determinations, CMS evaluates relevant clinical evidence to determine whether or not the evidence is of sufficient quality to support a finding that an item or service is reasonable and necessary. The overall objective for the critical appraisal of the evidence is to determine to what degree we are confident that: 1) the specific assessment questions can be answered conclusively; and 2) the intervention will improve health outcomes for patients.
We divide the assessment of clinical evidence into three stages: 1) the quality of the individual studies; 2) the generalizability of findings from individual studies to the Medicare population; and 3) overarching conclusions that can be drawn from the body of the evidence on the direction and magnitude of the intervention’s potential risks and benefits.
The methodological principles described below represent a broad discussion of the issues we consider when reviewing clinical evidence. However, it should be noted that each coverage determination has its unique methodological aspects.
Assessing Individual Studies
Methodologists have developed criteria to determine weaknesses and strengths of clinical research. Strength of evidence generally refers to: 1) the scientific validity underlying study findings regarding causal relationships between health care interventions and health outcomes; and 2) the reduction of bias. In general, some of the methodological attributes associated with stronger evidence include those listed below:
- Use of randomization (allocation of patients to either intervention or control group) in order to minimize bias.
- Use of contemporaneous control groups (rather than historical controls) in order to ensure comparability between the intervention and control groups.
- Prospective (rather than retrospective) studies to ensure a more thorough and systematical assessment of factors related to outcomes.
- Larger sample sizes in studies to demonstrate both statistically significant as well as clinically significant outcomes that can be extrapolated to the Medicare population. Sample size should be large enough to make chance an unlikely explanation for what was found.
- Masking (blinding) to ensure patients and investigators do not know to that group patients were assigned (intervention or control). This is important especially in subjective outcomes, such as pain or quality of life, where enthusiasm and psychological factors may lead to an improved perceived outcome by either the patient or assessor.
Regardless of whether the design of a study is a randomized controlled trial, a non-randomized controlled trial, a cohort study or a case-control study, the primary criterion for methodological strength or quality is to the extent that differences between intervention and control groups can be attributed to the intervention studied. This is known as internal validity. Various types of bias can undermine internal validity. These include:
- Different characteristics between patients participating and those theoretically eligible for study but not participating (selection bias).
- Co-interventions or provision of care apart from the intervention under evaluation (performance bias).
- Differential assessment of outcome (detection bias).
- Occurrence and reporting of patients who do not complete the study (attrition bias).
In principle, rankings of research design have been based on the ability of each study design category to minimize these biases. A randomized controlled trial minimizes systematic bias (in theory) by selecting a sample of participants from a particular population and allocating them randomly to the intervention and control groups. Thus, in general, randomized controlled studies have been typically assigned the greatest strength, followed by non-randomized clinical trials and controlled observational studies. The design, conduct and analysis of trials are important factors as well. For example, a well-designed and conducted observational study with a large sample size may provide stronger evidence than a poorly designed and conducted randomized controlled trial with a small sample size. The following is a representative list of study designs (some of that have alternative names) ranked from most to least methodologically rigorous in their potential ability to minimize systematic bias:
Randomized controlled trials
Non-randomized controlled trials
Prospective cohort studies
Retrospective case control studies
Cross-sectional studies
Surveillance studies (e. g., using registries or surveys)
Consecutive case series
Single case reports
When there are merely associations but not causal relationships between a study’s variables and outcomes, it is important not to draw causal inferences. Confounding refers to independent variables that systematically vary with the causal variable. This distorts measurement of the outcome of interest because its effect size is mixed with the effects of other extraneous factors. For observational, and in some cases randomized controlled trials, the method in that confounding factors are handled (either through stratification or appropriate statistical modeling) are of particular concern. For example, in order to interpret and generalize conclusions to our population of Medicare patients, it may be necessary for studies to match or stratify their intervention and control groups by patient age or co-morbidities.
Methodological strength is, therefore, a multidimensional concept that relates to the design, implementation and analysis of a clinical study. In addition, thorough documentation of the conduct of the research, particularly study selection criteria, rate of attrition and process for data collection, is essential for CMS to adequately assess and consider the evidence.
Generalizability of Clinical Evidence to the Medicare Population
The applicability of the results of a study to other populations, settings, treatment regimens and outcomes assessed is known as external validity. Even well-designed and well-conducted trials may not supply the evidence needed if the results of a study are not applicable to the Medicare population. Evidence that provides accurate information about a population or setting not well represented in the Medicare program would be considered but would suffer from limited generalizability.
The extent to that the results of a trial are applicable to other circumstances is often a matter of judgment that depends on specific study characteristics, primarily the patient population studied (age, sex, severity of disease and presence of co-morbidities) and the care setting (primary to tertiary level of care, as well as the experience and specialization of the care provider). Additional relevant variables are treatment regimens (dosage, timing and route of administration), co-interventions or concomitant therapies, and type of outcome and length of follow-up.
The level of care and the experience of the providers in the study are other crucial elements in assessing a study’s external validity. Trial participants in an academic medical center may receive more or different attention than is typically available in non-tertiary settings. For example, an investigator’s lengthy and detailed explanations of the potential benefits of the intervention and/or the use of new equipment provided to the academic center by the study sponsor may raise doubts about the applicability of study findings to community practice.
Given the evidence available in the research literature, some degree of generalization about an intervention’s potential benefits and harms is invariably required in making coverage determinations for the Medicare population. Conditions that assist us in making reasonable generalizations are biologic plausibility, similarities between the populations studied and Medicare patients (age, sex, ethnicity and clinical presentation) and similarities of the intervention studied to those that would be routinely available in community practice.
A study’s selected outcomes are an important consideration in generalizing available clinical evidence to Medicare coverage determinations. One of
the goals of our determination process is to assess health outcomes. These outcomes include resultant risks and benefits such as increased or decreased morbidity and mortality. In order to make this determination, it is often necessary to evaluate whether the strength of the evidence is adequate to draw
conclusions about the direction and magnitude of each individual outcome relevant to the intervention under study. In addition, it is important that an
intervention’s benefits are clinically significant and durable, rather than marginal or short-lived. Generally, an intervention is not reasonable and necessary if its risks outweigh its benefits.
If key health outcomes have not been studied or the direction of clinical effect is inconclusive, we may also evaluate the strength and adequacy of indirect evidence linking intermediate or surrogate outcomes to our outcomes of interest.
Assessing the Relative Magnitude of Risks and Benefits
Generally, an intervention is not reasonable and necessary if its risks outweigh its benefits. Health outcomes are one of several considerations in determining whether an item or service is reasonable and necessary. CMS places greater emphasis on health outcomes actually experienced by patients, such as quality of life, functional status, duration of disability, morbidity and mortality, and less emphasis on outcomes that patients do not directly experience, such as intermediate outcomes, surrogate outcomes, and laboratory or radiographic responses. The direction, magnitude, and consistency of the risks and benefits across studies are also important considerations. Based on the analysis of the strength of the evidence, CMS assesses the relative magnitude of an intervention or technology’s benefits and risk of harm to Medicare beneficiaries.
APPENDIX B
Medicare National Coverage Determinations Manual
This information is representative of Medicare's national coverage determination (NCD) for implementation purposes only. The information is subject to formal revisions and formatting changes prior to the release of the final NCD contractor instructions and publication in the Medicare National Coverage Determinations Manual.
Table of Contents
(Rev.)
[XXX.X]
A. General
Ambulatory blood pressure monitoring (ABPM) is a diagnostic test that allows for the identification of various types of high blood pressure. ABPM devises are small portable machines that are connected to a blood pressure cuff worn by patients that record blood pressure at regular periods over 24 to 48 hours while the patient goes about their normal activities, including sleep. The recording is interpreted by a physician or non-physician practitioner, and appropriate action is taken based on the findings. Diagnosis and treatment of high blood pressure is important for the management of various conditions including cardiovascular disease and kidney disease.
B. Nationally Covered Indications
The Centers for Medicare & Medicaid Services (CMS) has determined that the evidence is sufficient to determine that ambulatory blood pressure monitoring (ABPM) is reasonable and necessary for the diagnosis of hypertension in Medicare beneficiaries under the following circumstances:
- For beneficiaries with suspected white coat hypertension, which is defined as an average office blood pressure of systolic blood pressure greater than 130 mm Hg but less than 160 mm Hg or diastolic blood pressure greater than 80 mm Hg but less than 100 mm Hg on two separate clinic/office visits with at least two separate measurements made at each visit and with at least two blood pressure measurements taken outside the office which are <130/80 mm Hg.
- For beneficiaries with suspected masked hypertension, which is defined as average office blood pressure between 120 mm Hg and 129 mm Hg for systolic blood pressure or between 75 mm Hg and 79 mm Hg for diastolic blood pressure on two separate clinic/office visits with at least two separate measurements made at each visit and with at least two blood pressure measurements taken outside the office which are ≥130/80 mm Hg.
ABPM devices must be:
- capable of producing standardized plots of blood pressure measurements for 24 hours with daytime and night-time windows and normal blood pressure bands demarcated;
- provided to patients with oral and written instructions and a test run in the physician’s office must be performed; and
- interpreted by the treating physician or treating non-physician practitioner.
For eligible patients, ABPM is covered once per year.
C. Other Indications
Coverage of other indications for ABPM are at the discretion of the Medicare Administrative Contractors.
D. Other
(none)
APPENDIX C
Current Section 20.19 of the National Coverage Determination Manual
Item/Service Description
Ambulatory blood pressure monitoring (ABPM) involves the use of a non-invasive device which is used to measure blood pressure in 24-hour cycles. These 24-hour measurements are stored in the device and are later interpreted by the physician.
Indications and Limitations of Coverage
ABPM must be performed for at least 24 hours to meet coverage criteria.
ABPM is only covered for those patients with suspected white coat hypertension. Suspected white coat hypertension is defined as:
- Office blood pressure >140/90 mm Hg on at least three separate clinic/office visits with two separate measurements made at each visit;
- At least two documented blood pressure measurements taken outside the office which are <140/90 mm Hg; and
- No evidence of end-organ damage.
The information obtained by ABPM is necessary in order to determine the appropriate management of the patient. ABPM is not covered for any other uses. In the rare circumstance that ABPM needs to be performed more than once in a patient, the qualifying criteria described above must be met for each subsequent ABPM test.
For those patients that undergo ABPM and have an ambulatory blood pressure of <135/85 with no evidence of end-organ damage, it is likely that their cardiovascular risk is similar to that of normotensives. They should be followed over time. Patients for which ABPM demonstrates a blood pressure of >135/85 may be at increased cardiovascular risk, and a physician may wish to consider antihypertensive therapy.


