TO: Administrative File: CAG-00454N
FROM: Tamara Syrek Jensen, JD
Director, Coverage and Analysis Group
Joseph Chin, MD, MS
Deputy Director, Coverage and Analysis Group
Melissa A. Evans, PhD, MSAE
Director, Division of Policy & Evidence Review
Lori Ashby, MA
Deputy Director, Division of Policy & Evidence Review
Carl Li, MD, MPH
Lead Medical Officer
Kimberly Long
Lead Analyst
SUBJECT: National Coverage Determination for Screening for Colorectal Cancer-Blood-Based Biomarker Tests
DATE: January 19, 2021
I. Decision
The Centers for Medicare & Medicaid Services (CMS) has determined that the evidence is sufficient to cover a blood-based biomarker test as an appropriate colorectal cancer screening test once every 3 years for Medicare beneficiaries when performed in a Clinical Laboratory Improvement Act (CLIA)-certified laboratory, when ordered by a treating physician and when all of the following requirements are met:
The patient is:
- age 50-85 years, and,
- asymptomatic (no signs or symptoms of colorectal disease including but not limited to lower gastrointestinal pain, blood in stool, positive guaiac fecal occult blood test or fecal immunochemical test), and,
- at average risk of developing colorectal cancer (no personal history of adenomatous polyps, colorectal cancer, or inflammatory bowel disease, including Crohn’s Disease and ulcerative colitis; no family history of colorectal cancers or adenomatous polyps, familial adenomatous polyposis, or hereditary nonpolyposis colorectal cancer).
The blood-based biomarker screening test must have all of the following:
- FDA market authorization with an indication for colorectal cancer screening; and
- proven test performance characteristics for a blood-based screening test with both sensitivity greater than or equal to 74% and specificity greater than or equal to 90% in the detection of colorectal cancer compared to the recognized standard (accepted as colonoscopy at this time), based on the pivotal studies included in the FDA labeling.
The currently available Epi proColon® test does not meet the criteria for an appropriate blood-based biomarker CRC screening test. Based on the evidence at this time, we will non-cover the Epi proColon® test.
See Appendix B for the draft manual language.
II. Background
Throughout this document, we use numerous acronyms, some of which are not defined as they are presented in direct quotations. Please find below a list of these acronyms and corresponding full terminology. Additionally, nomenclature for DNA gene markers is used throughout this document. Gene names are expressed in italics.
AA – advanced adenoma
ACG – American College of Gastroenterology
ACS – American Cancer Society
CI – confidence interval
CISNET - Cancer Intervention and Surveillance Modeling Network
CMS – Centers for Medicare & Medicaid Services
CRC – colorectal cancer
ctDNA - circulating tumor DNA
DNA – deoxyribonucleic acid
fDNA – fecal deoxyribonucleic acid
FOBT – fecal occult blood test
FDA – United States Food & Drug Administration
FIT – fecal immunochemical test
gFOBT - guaiac-based fecal occult blood test
HP - hyperplastic polyps
HP2020 – Healthy People 2020
MEDCAC – Medicare Evidence Development & Coverage Advisory Committee
MMR - mismatch repair
mSEPT9 - methylated SEPT9
mts-DNA - multitarget stool DNA
NCA - National Coverage Analysis
NCD - National Coverage Determination
NCI – National Cancer Institute
NCCN - National Comprehensive Cancer Network
NED – no evidence of disease
NIH – National Institutes of Health
NNS – number needed to screen
OS – overall survival
PCR - polymerase chain reaction
PDR - positive detection rate
PFS – progression free survival
QuARTS – quantitative allele-specific real-time target and signal amplification
RT-PCR - reverse transcription polymerase chain reaction
sDNA – stool deoxyribonucleic acid
SEER – Surveillance, Epidemiology, and End Results
SP - small polyps
SSA – sessile serrated adenoma
SSED – Summary of Safety and Effectiveness Data
SSP – sessile serrated polyps
TCGA - The Cancer Genome Atlas
UICC - Union for International Cancer Control
US - United States
USMSTF – United States Multi-Society Task Force
USPSTF – United States Preventive Services Task Force
CMS initiated this national coverage determination (NCD) to consider coverage for colorectal cancer (CRC) screening using a blood-based biomarker test. While we have focused our review on commercially available tests, we recognize there may be other blood-based biomarker screening tests available in the future and thus have included a more general analysis and discussion.
CRC is the fourth most common cancer and the second leading cause of cancer deaths in the United States (NIH/SEER 2020). It is an important issue for the Medicare population. In 2020, the National Institutes of Health (NIH) National Cancer Institute (NCI) estimated that there will be over 147,000 new cases of colon and rectum cancer in the United States with a median age at diagnosis of 67 years (NIH/SEER 2020). Colorectal cancer is most frequently diagnosed among people aged 65 – 74 years (NIH/SEER 2020).
Overall mortality rates for CRC have declined over the past decade (NIH/SEER 2020). The death rate for CRC has dropped by 53% from 1970 to 2016 (Siegel, 2019). Primary prevention, early detection and early treatment have contributed to the observed reduction in mortality (Siegel, 2019); however, CRC was estimated to account for over 53,000 deaths in 2020, with a median age at death of 74 years (NIH/SEER 2020). For colorectal cancer, death rates increase with age, with the percent of colorectal cancer deaths highest among people aged 75-84 years in 2020. The CRC death rate is slightly higher for men compared to women. Among all races, African-Americans have the highest death rate (NIH/SEER 2020). Based on data from SEER 18 2010-2016, the five-year relative survival rate was 64.6% (NIH/SEER 2020).
The natural history of colorectal neoplasia has been well studied.
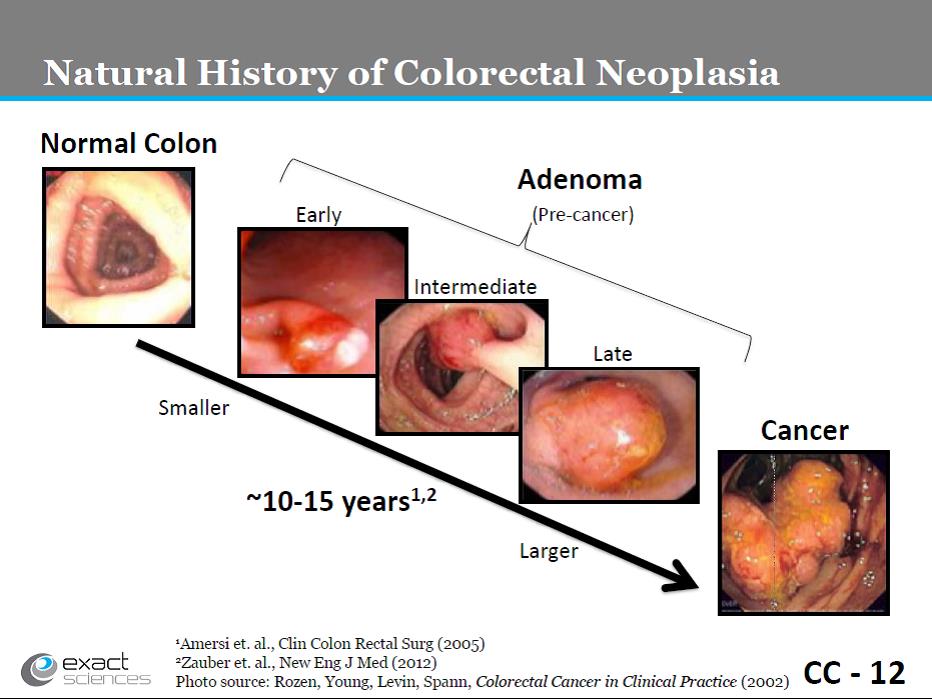
(Slide CC-12. Exact Sciences presentation, March 27, 2014.K
Exact Sciences Corp. Cologuard Presentation at FDA Molecular and Clinical Genetics Panel. March 27, 2014.
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/MedicalDevices/MedicalDevicesAdvisoryCommittee/MolecularandClinic
Percent of Cases & 5-Year Relative Survival by Stage at Diagnosis: Colorectal Cancer
Percent of Cases by Stage
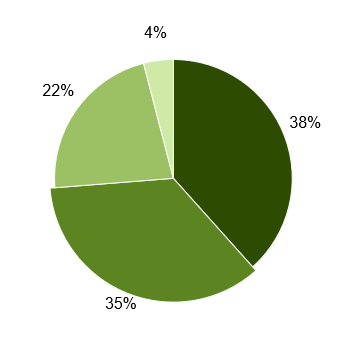
 Localized (38%)
Localized (38%)
Confined to Primary Site
 Regional (35%)
Regional (35%)
Spread to Regional Lymph Nodes
 Distant (22%)
Distant (22%)
Cancer Has Metastasized
 Unknown (4%)
Unknown (4%)
Unstaged
5-Year Relative Survival
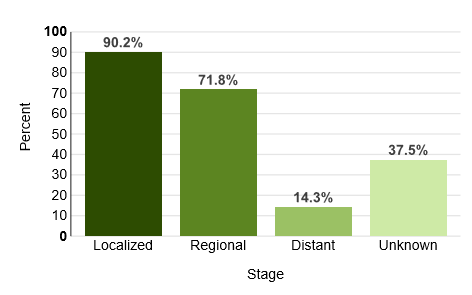
Percent of Cases & 5-Year Relative Survival by Stage at Diagnosis: Colorectal Cancer. https://seer.cancer.gov/statfacts/html/colorect.html, accessed 07/26/2020.
Fecal Occult Blood Test (FOBT) and Fecal Immunoassay Test (FIT)
Early detection through screening for colorectal cancer has been shown to improve mortality (Mandel, 1993; Nishihara, 2013; Shaukat, 2013). Non-invasive colorectal cancer (CRC) screening tools include fecal occult blood testing (FOBT) and immunochemical-based fecal occult blood testing (FIT). Through 30 years of follow-up in the randomized controlled Minnesota Colon Cancer Control Study, annual screening with fecal occult-blood testing (FOBT) reduced colorectal cancer mortality by 32% (Shaukat, 2013). An organized CRC screening outreach program that consisted primarily of annual fecal immunochemical testing (FIT) and colonoscopy was implemented in a large, community-based population in California starting in 2007 through 2008. Comparing mortality rates before the screening outreach program (baseline year 2000) to after (through 2015) implementation resulted in a statistically significant increased screening participation rate, primarily due to increased uptake of FIT and colonoscopy. The increased screening was associated with a statistically significant decrease in CRC incidence and mortality (Levin, 2018). The analysis was not stratified by screening modality so there was no data on the association of uptake of FIT alone and CRC mortality. The evidence suggests that there is clinical utility in using FOBT and FIT for early detection of colorectal cancer (CRC) which reduces mortality of the disease.
Advanced Adenoma
Early detection of large pre-cancerous adenomas and removal prevents progression of these adenomas to carcinoma, reducing the incidence of colorectal cancer (Mandel, 2000; Nishihara, 2013).
Screening
Mortality from CRC has decreased over the past 20 years due in large part to an increase in recommendation consistent screening. Since the 1990s, Medicare has covered a number of CRC screening tests from non-invasive fecal based tests to colonoscopy, providing a range of choices for patients to choose the most individually suitable modalities. Screening rates for Medicare beneficiaries have been consistently higher than the general recommended target group. The Centers for Disease Prevention and Control reports CRC screening rates based upon results of the Behavioral Risk Factor Surveillance System. For example, in 2018, the adults who were up to date with CRC screening tests was 63.3% for individuals aged 50-64 years and 79.2% for individuals aged 65-75 years (overall 68.8%; Joseph et al., 2020 at https://www.cdc.gov/mmwr/volumes/69/wr/mm6910a1.htm, accessed 07/26/2020).
Blood-Based Biomarker Testing
Over the last several years, blood-based biomarker tests, one example is the Epi proColon® test; have emerged as another potential non-invasive option for the early detection of colorectal cancer. While the Epi proColon® test is the only FDA-approved blood-based biomarker test for colorectal cancer screening at the time of this analysis, there are other blood-based tests in development using different biomarkers. A blood-based biomarker (biological marker in the patient’s blood) is a measurable DNA, RNA or protein component that indicates disease, in this case cancer. For example, blood-based cancer biomarkers include but are not limited to specific gene mutations, methylation of genes, and antigens. The blood-based biomarker that is measured in a person’s blood can be an indicator of a process, such as disease risk or progression, like progression to colorectal cancer, thought to be correlated with a long term outcome, such as mortality. It is typically easier to measure a biomarker than the true outcome of interest, such as mortality from colorectal cancer. However, the biomarker might not be a good surrogate for and not well correlated with the clinical outcome of interest, such as cancer survival or mortality, or it might not identify a patient early enough to alter the clinical course of disease.
Blood-based biomarker (such as DNA alteration) testing detects molecular markers of altered DNA or RNA (Christou, 2019), or perhaps even in the future proteins, that are contained in the cells shed into the lumen of the large bowel by CRC and pre-malignant colorectal epithelial neoplasia. With the discrete natural history of colorectal neoplasia, several events during the development and progression of adenomas to CRC have been identified and classified including: (1) mutational activation of proto-oncogenes (normal genes that are involved in cellular growth and proliferation); (2) mutational inactivation of tumor suppressor genes (normal genes that suppress cellular growth and proliferation); (3) specific chromosomal point mutations; and (4) accumulation of sufficient genetic alterations for tumorigenesis (Vogelstein, 1988; Friend, 1988; Fearon, 1990; Cho, 1992).
The biologic mechanism underlying colorectal cancer involves various genetic and epigenetic alterations in intestinal epidermal cells. As an example, while DNA methylation is one of the molecular markers essential for the regulation of gene expression, epigenetic changes resulting from altered DNA methylation can have an important role in tumorigenesis. DNA methylation is a biological process by which methyl (CH3) groups are added to the DNA molecule. Epigenetic transcriptional changes are changes in gene expression without DNA sequence changes. Aberrant DNA methylation of the 5’-Cytosine-phosphate-Guanine-3’ (C-phosphate-G or CpG) site in promoter regions of genes has been linked to epigenetic transcriptional silencing of tumor suppressor genes, which appears to be crucial in the early stages of CRC development (Xie, 2018).
The SEPT9, also called Septin9, gene is one of several genes involved in cellular proliferation control (Galanopoulos, 2017), such as cytokinesis and cell control of biological processes such as division of cytoplasm, cell polarization, vesicle transport, and membrane reconstruction. The septin-9 protein also appears to act as a tumor suppressor, which means that it regulates cell growth and prevents cells from dividing too fast or in an uncontrolled way. When the SEPT9 gene is unmethylated, the unmethylated CpG islands gives rise to active gene transcription of the SEPT9 gene which suppresses the tumor. When the SEPT9 gene is methylated, the methylated CpG islands inactivate epigenetic transcription of the SEPT9 gene, inactivating or silencing the tumor suppressor SEPT9 gene. Thus, methylation of the SEPT9 gene triggers cellular progression towards malignancy in the colon mucosa leading to colorectal cancer development.
Aberrant hypermethylation of the SEPT9 gene gives rise to methylated Septin9, or mSEPT9, which is a DNA methylation-based molecular biomarker that encodes Septin-9 and has been associated with CRC. The mSEPT9 gene DNA, located at chromosome 17, is involved in cytokinesis and cytoskeletal organization in the cell. SEPT9 is closely related to CRC carcinogenesis since the cytosine base pairs in the promoter region of the SEPT9 gene V2 transcript are hypermethylated. mSEPT9 gene DNA is released into the peripheral circulating blood, i.e., the circulating tumor DNA or ctDNA, from necrotic and apoptotic cancer cells during CRC carcinogenesis. mSEPT9 can be detected in blood plasma (Xie, 2018). These fragments of DNA are representative of cancer cells in the tumor tissue. Aberrant hypermethylation of V2 transcript of SEPT9 gene has been observed in almost 100% of CRC diseased subjects (Hu, 2019). This region is generally unmethylated in samples from non-diseased subjects (FDA, FDA Executive Summary on Epi proColon®, March 26, 2014). The risk of CRC can be estimated by detecting the degree of DNA methylation of the specific promoter region of SEPT9 in the peripheral blood. Thus methylation of target DNA sequence in the promoter region of SEPT9 v2 transcript is associated with colorectal cancer.
One example test, Epi proColon®, functions as a blood-based colorectal cancer screening test by identifying the circulating mSEPT9 (Septin9) gene in cell-free DNA isolated from plasma. CRC tumors have an increased likelihood of exhibiting aberrant methylation at the promoter region of the SEPT9 gene DNA (Hariharan, 2020). This test is a qualitative in vitro diagnostic test for the detection of methylated Septin 9 DNA in EDTA plasma derived from patient whole blood specimens. The test process consists of real-time polymerase chain reaction (PCR) wtih a fluorescent hydrolysis probe for methylation specific detection of Septin 9 DNA target. The Epi proColon® testing procedure involves optimized sample processing and proprietary assay methodologies for the detection of the mSEPT9 biomarker in blood. It is a qualitative real-time assay in which each sample is tested in triplicate runs during PCR analysis (Yan, 2016). Currently, this test is the only FDA approved commercially available blood-based CRC screening test that is marketed in the US.
As with other noninvasive fecal CRC screening tests (guaiac fecal occult blood tests (FOBT), FIT), referral following a positive blood-based colorectal screening test to a diagnostic and often therapeutic (if lesions are removed) colonoscopy is essential to reduce incidence of and mortality from CRC.
III. History of Medicare Coverage
Sections 1861(s)(2)(R) and 1861(pp) of the Act authorize coverage for screening colorectal cancer tests under Medicare Part B. Among other things, the statute enables the Secretary to add coverage for “other tests and procedures, and modifications to tests and procedures under this subsection, with such frequency and payment limits, as the Secretary determines appropriate, in consultation with appropriate organizations.” (Section 1861(pp)(1)(D) of the Act; 42 CFR 410.37(a)(1)(v)). Our regulations can be found at 42 CFR 410.37.
In the Physician Fee Schedule Final Rule for 2003, CMS amended the FOBT screening test regulation definition in 42 CFR 410.37(a)(2) to provide that it could include coverage of either (1) a guaiac-based FOBT, or (2) other tests as determined by the Secretary through a national coverage determination (67 Fed. Reg. 79966, 80040) (December 31, 2002). On November 4, 2003, CMS issued a final Decision Memorandum indicating that effective with that date Medicare would cover a screening fecal immunoassay test (FIT) (See Pub. 100-03, Chapter 1, Section 210.3, screening immunoassay FOBT) on an annual basis as an alternative to the guaiac-based FOBT.
In the Physician Fee Schedule Final Rule for 2003, CMS also amended the colorectal cancer screening test regulation in 42 CFR 410.37(a)(1)(v) to provide that in addition to the screening test options already covered under the regulation, it could include coverage of additional colorectal cancer screening tests through issuance of a national coverage determination (67 Fed. Reg. 79966, 80040) (December 31, 2002).
Medicare currently covers the following CRC screening tests for beneficiaries that meet certain frequency and eligibility criteria: (1) screening FOBT, (2) screening flexible sigmoidoscopy, (3) screening colonoscopy, (4) screening barium enema as an alternative to flexible sigmoidoscopy or colonoscopy, (5) Cologuard™ – a multi-target sDNA colorectal cancer screening test, and (6) other tests and procedures and modifications to such tests and procedures the Secretary determines appropriate in consultation with appropriate organizations.
A. Current Request
CMS received a formal request for a national coverage determination from Epigenomics, to consider coverage of Epi proColon®-a blood-based screening test. The formal request letter can be viewed via the tracking sheet for this NCA on the CMS website at: https://www.cms.gov/medicare-coverage-database/details/nca-details.aspx?NCAId=299
B. Benefit Category
Medicare is a defined benefit program. For an item or service to be covered by the Medicare program, it must fall within one of the statutorily defined benefit categories outlined in the Social Security Act. Congress has specifically authorized coverage of certain screening tests under Part B of the Medicare program. CRC screening tests have a benefit category under §1832, §1861(s)(2)(R) and §1861(pp) of the Act. Specifically, we are using the national coverage determination authority under section 1861(pp)(1)(D) (and implementing regulations at 42 CFR 410.37(a)(1)(v)) to determine whether the scope of the CRC screening benefit should be expanded to include coverage of blood-based
screening tests.
IV. Timeline of Recent Activities
| Date |
Action |
|---|
February 28, 2020 |
CMS posts a tracking sheet announcing the opening of the NCA. The initial 30-day comment period begins. |
March 10, 2020 |
Epigenomics met with CMS to discuss their NCD request. |
March 29, 2020 |
First public comment period ends. CMS receives 67 comments. |
| October 16, 2020 |
Proposed Decision Memorandum posted. 30-day public comment period begins. |
| November 15, 2020 |
30-day public comment period ends. CMS receives 173 comments. |
V. Food and Drug Administration (FDA) Status
The Epi proColon® test is a FDA-approved test with the following Intended Use and Indications for Use.
Intended Use:
The Epi proColon® test is a qualitative in vitro diagnostic test for the detection of methylated Septin 9 DNA in EDTA plasma derived from patient whole blood specimens. Methylation of the target DNA sequence in the promoter region of the SEPT9_v2 transcript has been associated with the occurrence of colorectal cancer (CRC). The test uses a real-time polymerase chain reaction (PCR) with a fluorescent hydrolysis probe for the methylation specific detection of the Septin 9 DNA target. The Epi proColon® test is indicated to screen adults of either sex, 50 years or older, defined as average risk for CRC, who have been offered and have a history of not completing CRC screening. Tests that are available and recommended in the USPSTF 2008 CRC screening guidelines should be offered and declined prior to offering the Epi proColon® test. Patients with a positive Epi proColon® test result should be referred for diagnostic colonoscopy. The Epi proColon® test results should be used in combination with physician's assessment and individual risk factors in guiding patient management.
Contraindications:
- The Epi proColon® test is not intended to replace colorectal cancer screening tests that are recommended by appropriate guidelines (e.g., 2008 USPSTF guidelines) such as colonoscopy, sigmoidoscopy and high sensitivity fecal occult blood testing.
- The Epi proColon® test is not intended for patients who are willing and able to undergo routine colorectal cancer screening tests that are recommended by appropriate guidelines.
- The Epi proColon® test is not intended for patients defined as having elevated risk for developing CRC based on previous history of colorectal polyps, CRC or related cancers, inflammatory bowel disease (IBD), chronic ulcerative colitis (CUC), Crohn’s disease, familial adenomatous polyposis (FAP). Persons at higher risk also include those with a family history of CRC, particularly with two or more first degree relatives with CRC, or one or more first degree relative(s) less than 50 years of age with CRC.
- The Epi proColon® test has not been evaluated in patients who have been diagnosed with a relevant familial (hereditary) cancer syndrome, such as non-polyposis colorectal cancer (HNPCC or Lynch Syndrome), Peutz-Jeghers Syndrome, MYH-Associated Polyposis (MAP), Gardner’s syndrome, Turcot’s (or Crail’s) syndrome, Cowden’s syndrome, Juvenile Polyposis, Cronkhite Canada syndrome, Neurofibromatosis, or Familial Hyperplastic Polyposis, or in patients with anorectal bleeding, hematochezia, or with known iron deficiency anemia.
VI. General Methodological Principles
When making national coverage decisions concerning the scope of the CRC screening benefit under Medicare Part B, CMS evaluates relevant clinical evidence to determine whether or not the evidence is of sufficient quality to support a finding that a test is suitable and appropriate for general screening in individuals with no signs or symptoms of the condition being screened for in the Medicare population. A detailed account of the methodological principles of study design that the Agency utilizes to assess the relevant literature can be found in Appendix A. In general, features of clinical studies that improve quality and decrease bias include the selection of a clinically relevant cohort, the consistent use of a single good reference standard, the blinding of readers of the index test, and reference test results.
Public comments sometimes cite the published clinical evidence and give CMS useful information. Public comments that give information on unpublished evidence such as the results of individual practitioners or patients are less rigorous and therefore less useful for making a coverage determination. Public comments that contain personal health information (PHI) will be redacted and the PHI will not be made available to the public. CMS responds in detail to the public comments on a proposed decision when issuing the final decision memorandum.
VII. Evidence
A. Introduction
CMS has added several colorectal cancer screening tests in the past few years and have established a consistent analytic framework. The basic parameters for screening were established many years ago and are still well accepted to date. In 1968, Wilson and Jungner reported criteria to consider:
- The condition being screened for should be an important health problem,
- The natural history of the condition should be well understood,
- There should be a detectable early stage,
- Treatment at an early stage should be of more benefit than at a later stage,
- A suitable test should be devised for the early stage,
- The test should be acceptable,
- Intervals for repeating the test should be determined,
- Adequate health service provision should be made for the extra clinical workload resulting from screening,
- The risks, both physical and psychological, should be less than the benefits, and
- The costs should be balanced against the benefits.
(Wilson JMG, Jungner G. Principles and Practice of Screening for Disease. World Health Organization, 1968)
The evaluation of screening tests has been largely standardized in the medical and scientific communities, and the value of a screening test may be assessed according to the following criteria:
- “Simplicity. In many screening programmes more than one test is used to detect one disease, and in a multiphasic programme the individual will be subjected to a number of tests within a short space of time. It is therefore essential that the tests used should be easy to administer and should be capable of use by para-medical and other personnel.
- Acceptability. As screening is in most instances voluntary and a high rate of co-operation is necessary in an efficient screening programme, it is important that tests should be acceptable to the subjects.
- Accuracy. The test should give a true measurement of the attribute under investigation.
- Cost. The expense of screening should be considered in relation to the benefits resulting from the early detection of disease, i.e., the severity of the disease, the advantages of treatment at an early stage and the probability of cure.
- Precision (sometimes called repeatability). The test should give consistent results in repeated trials.
- Sensitivity. This may be defined as the ability of the test to give a positive finding when the individual screened has the disease or abnormality under investigation.
- Specificity. This may be defined as the ability of the test to give a negative finding when the individual screened does not have the disease or abnormality under investigation.”
(Cochrane A and Holland W. Validation of screening procedures. British Medical Bulletin 1971;27(1):3-8. PMID: 5100948).
There are a number of structured methods for evaluating screening tests. In past diagnostic imaging NCDs, we considered the evidence in the hierarchical framework of Fryback and Thornbury (1991) which has six levels of assessment.
- Level 1 concerns technical quality of the images;
- Level 2 addresses diagnostic accuracy, sensitivity, and specificity of the test;
- Level 3 focuses on whether the information produces change in the physician's diagnostic thinking;
- Level 4 concerns the effect on the patient management plan;
- Level 5 measures the effect of the diagnostic information on patient outcomes; and
- Level 6 examines societal costs and benefits of the diagnostic imaging technology.
In other NCDs on diagnostic tests, we generally looked for sound evidence that shows the test is analytically and clinically valid (Levels 1-2) and that use of the test to guide treatment is reasonable and necessary for improved health outcomes (clinical utility, Levels 3-5). In our analysis of screening tests, we will adapt the hierarchical framework of Fryback and Thornbury (1991) and generally look for sound evidence that shows the screening test is analytically and clinically valid (Levels 1-2).
Health outcomes, benefits, and risks are important considerations. As Cochrane and Holland (1971) further noted, evidence on health outcomes, for example, evidence that screening can alter the natural history of disease in a significant proportion of those screened," is important in the consideration of screening tests since individuals are asymptomatic and "the practitioner initiates screening procedures." Since a number of colorectal cancer screening tests are available and covered by Medicare, how a new test should be used and how it fits into current recommendations for screening should also be considered.
B. Discussion of Evidence
1. Evidence Question(s)
Question 1: Is the evidence sufficient to determine that a blood-based biomarker screening test (at the time of this review Epi proColon® is the only FDA approved commercially available blood-based biomarker screening test) is a suitable colorectal cancer screening test for prevention or early detection in Medicare beneficiaries?
Question 2: Is the evidence sufficient to determine that colorectal cancer screening using a blood-based biomarker screening test is appropriate for Medicare beneficiaries?
2. External Technology Assessments
CMS did not request an external technology assessment (TA) on this issue.
3. Internal Technology Assessment
Literature Search Methods
CMS typically considers a category of tests or devices, rarely making decisions on brand specific items; however, since the Epi proColon® test is the only FDA-approved commercially available blood-based colorectal cancer screening test at the time of this review, we focused our review and included a specific search for evidence on this test. CMS staff searched PubMed for publications from the period of 1999 to April 2020. General keywords included the DNA biomarker for the screening test, “mSEPT9”, and colorectal cancer. Publications that presented original data on screening with blood-based DNA testing were considered. Publications that had the terms “blood-based”, “plasma”, and “colorectal cancer” in the abstract were included. Keywords for the search included “blood-based’, “mSEPT9”, “SEPT9 DNA”, “SEPT9”, “Septin 9”, “Septin9”, “Septin 9 DNA”, “Epi proColon®”, and “colorectal cancer screening”. CMS staff searched the bibliographies of relevant publications for other pertinent studies. Abstracts, meeting presentations, reviews, animal studies, microsimulation modeling studies, mechanistic studies, and non-English publications were excluded. Studies with fewer than 10 cases and those not involving human subjects were excluded. The reviewed evidence was gathered from articles submitted by the requester and from the public comments and the PubMed literature search.
We found 19 investigations that met our inclusion criteria. The details of these investigations are summarized below.
Meta-analyses/Systematic reviews
Hariharan R, Jenkins M. Utility of the methylated SEPT9 test for the early detection of colorectal cancer: a systematic review and meta-analysis of diagnostic test accuracy. BMJ Open Gastroenterol. 2020 Feb 18;7(1):e000355.
The aim of the systematic review was to conduct an updated meta-analysis to establish the sensitivity, specificity and accuracy of mSEPT9 tests for the early diagnosis of CRC, and have the results stratified by the region of recruitment, sample size and stage, and to evaluate the accuracy of a range of positivity thresholds for the mSEPT9 test. This systematic review and meta-analysis was conducted as per Guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis. A systematic search of the relevant literature was conducted using Medline and Embase databases. The authors stated that “the search was divided into three phases. All articles included in these databases from January 1946 to May 2018 were considered. The search terms for the first phase were: (‘colon’ or ‘colorectal’) and (‘cancer’ or ‘carcinoma’) and (‘serum’ or ‘plasma’) and ‘sensitivity’ and ‘specificity’. The search terms for the second phase were: (‘SEPT9’ or ‘SEPT9’ or ‘Septin-9’ or ‘mSEPT9’) and (‘colon’ or ‘colorectal’) and (‘methylated’ or ‘methylation’). The search terms for the third phase were: ‘Epi proColon®’ and ‘SEPT9’ and ‘diagnosis’.”
The publication stated that “the inclusion criteria were: full-text available, English language, human studies, case-control study design, CRC diagnosis either prior or following mSEPT9 test, report of sufficient data to enable construction of 2×2 tables of mSEPT9 result and CRC status, and the use of a mSEPT9 single gene assay for both cases and controls. Exclusion criteria were: articles that were meta-analysis, conference and meeting abstracts, studies that used a multigene ctDNA panel; and studies with <20 CRC case participants.” Data were extracted from the eligible studies and analyzed to estimate pooled sensitivity, specificity and diagnostic test accuracy, such as positive likelihood ratio, negative likelihood ratio, diagnostic ORs. The authors reported that positive predictive value (PPV) and negative predictive value (NPV) “were calculated assuming a CRC prevalence of 0.3% for an average risk population (consistent with having no first-degree relatives with CRC) and a CRC prevalence of 1.2% for a high-risk population (consistent with having two first-degree relatives with CRC). The range of threshold levels signifying a positive test were considered using either ‘one positive count out of three PCR results (1/3 algorithm)’ or ‘two positive counts out of three PCRs (2/3 algorithm)’, for the stratified subgroup analysis and meta-regression.”
Among the 19 studies, some were located in the US (6 studies) while others were located in Germany (2), Hungary (2), Denmark (1), China (5), South Korea (1), Singapore (1), and Taiwan (1). The 19 selected studies had a total of 7629 cases and controls. The individual study sample sizes ranged from 52 to 1544. The authors found that “of the 19 studies, 12 were screening studies (blood sample for mSEPT9 test taken prior to CRC diagnosis) and 7 were clinical studies (blood sample for mSEPT9 test after CRC diagnosis)….Fifteen studies collected plasma samples from participants for the mSEPT9 test prior to starting neoadjuvant therapy, adjuvant chemotherapy, radiotherapy or surgical resection and 17 studies confirmed CRC status by gold standard histopathology.” No other information on study design was provided, such as whether the studies were rospective or retrospective, the cases to controls ratio, or whether the screening studies and clinical studies were nested case-control studies. All CRC cases were diagnosed and staged before treatment. Among controls (individuals with no evidence of CRC), most (94.3%) were confirmed by prior colonoscopy. No sociodemographic information was provided. No information on the type of mSEPT9 test or whether they were FDA approved tests was provided.
The authors reported that “Based on 19 studies, the results revealed that the pooled estimates for mSEPT9 to detect CRC were: sensitivity 69% (95% CI: 62–75); specificity 92% (95% CI: 89–95); positive likelihood ratio 9.1 (95% CI: 6.1–13.8); negative likelihood ratio 0.34 (95% CI: 0.27–0.42); diagnostic odds ratio (OR) 27 (95% CI: 15–48) and area under the curve 0.89 (95% CI: 0.86–0.91).” The investigators found considerable heterogeneity for both sensitivity (I2=88.37%) and specificity (I2=96.29%). In an average risk population (0.3% CRC prevalence), the test has a positive predictive value of 2.6%; however, and negative predictive value of 99.9%, in a high-risk population with a 1.2% CRC prevalence, the test had a 9.5% positive predictive value and 99.6% negative predictive value. The 2/3 algorithm for positivity threshold had a similar sensitivity to the 1/3 threshold (2/3 = 0.69, 1/3 = 0.68). However, it had a higher specificity (2/3 = 0.95, 1/3 = 0.88) and a higher positive likelihood ratio (2/3 = 14.6, 1/3 = 5.7) and diagnostic OR (2/3 = 44, 1/3 = 16), with a lower negative likelihood ratio (2/3 = 0.33, 1/3 = 0.36).
The authors reported that “there was marginal evidence (p=0.06) for the heterogeneity in sensitivity being attributable to differences in sensitivity in North American studies and studies that recruited more cases with stage 1 CRC than cases with stage 4 CRC (p=0.06). There was strong evidence (p<0.01) that the heterogeneity in specificity was largely affected by size of study, and whether it was conducted in Asian (p<0.01) or North American (p<0.001) regions. Studies with a high proportion of stage 1 CRCs had a lower sensitivity (p=0.06) than those with a high proportion of stage 4 CRCs. There was marginal evidence of publication bias (p=0.05)”.
The authors acknowledged that “limitations of this meta-analysis included inability to investigate other non-threshold effects on heterogeneity or variations in PCR methodology and technology.”
The authors concluded that “the mSEPT9 test has high specificity and moderate sensitivity for CRC and is therefore a potential alternative screening method for those declining fecal immunochemical test for occult blood (FIT) or other screening modalities. However, it is limited by its poor diagnostic performance for precancerous lesions (advanced adenomas and polyps) and its relatively high costs, and little is known about its acceptability to those declining to use the FIT.” Further, they “observed marginal evidence that some of heterogeneity could be due to varying ctDNA positivity thresholds inferring that test accuracy depended on the positivity algorithm, with the optimum threshold level being the 2/3 algorithm. The North American studies had overall lower pooled diagnostic accuracy indicators potentially due to different positivity threshold used in that region.” The authors also concluded that “while mSEPT9 has diagnostic performance similar (although lower) to the FIT, it is currently unsuitable as its replacement in screening programmes.”
Hu J, Hu B, Gui YC, et al. Diagnostic Value and Clinical Significance of Methylated SEPT9 for Colorectal Cancer: A Meta-Analysis. Med Sci Monit. 2019 Aug 5;25:5813-5822.
The aim of the study was to conduct a comprehensive meta-analysis using all eligible published articles, to clarify the diagnostic role of plasma methylated SEPT9 (mSEPT9) in colorectal cancer (CRC) and to examine its association with CRC. The investigators conducted a search using the electronic databases PubMed, Cochrane Library, Web of Science, Google Scholar, and Chinese National Knowledge Infrastructure (CNKI), to identify eligible articles published before July 2018. The authors stated that the “following search terms were used: “colorectal cancer” or “CRC,” “methylated SEPT9” or “mSEPT9,” and “diagnosis” or “diagnose.” Included articles were limited to human studies, but not limited by language. Relevant articles were also searched using the related articles function in PubMed. In addition, references within the identified articles were also searched manually. The study was approved by the Review Boards of the First Affiliated Hospital of Guangxi Medical University. The inclusion criteria were as follows: (1) CRC was pathologically diagnosed and none of the patients received chemotherapy, radiotherapy, or surgical intervention before colonoscopy examination; (2) studies that analyzed the diagnostic value of plasma mSEPT9 for CRC using a defined test method; and (3) the sensitivity and specificity data of mSEPT9 for CRC were provided. The exclusion criteria were as follows: review articles, letters, case reports and studies on cell lines, non-plasma/non-serum samples, unknown detection methods, and animal experiments. When the same patient cohort was reported in several articles, the most recent study was selected.”
Summary sensitivity, specificity, positive and negative likelihood ratio (PLR/NLR), and diagnostic odds ratio (DOR) were calculated for the diagnostic value of mSEPT9 for CRC. The area under the receiver operating curve (AUC) was used to summarize the overall test performance.
All studies were prospective and included CRC patients that were confirmed by pathological diagnosis. Overall, 22 studies with 2271 subjects (1801 CRC patients and 470 controls) were included in the meta-analysis. The mean age of patients by study ranged from 52.5 years to 71 years. Testing methods for mSEPT9 included the Epi proColon® test 1.0 (six studies), Epi proColon® test 2.0 (eight studies), and reverse transcription polymerase chain reaction (RT-PCR) assay (eight studies). Among the RT-PCR assays, all eight were research kits and were not FDA approved. Five studies provided data for FIT (two studies) or FOBT (three studies) in the diagnosis of CRC. Nine studies were located in China, six in Germany, five in the United States, one in Korea, and one in Denmark. There was significant heterogeneity in the summary sensitivity (I2=84.5%, p<0.001) and specificity (I2=88.8%, p<0.001). No publication bias was found across the studies using Deek’s test (p=0.653).
For the results, the summary sensitivity and specificity of mSEPT9 were 0.69 (95% confidence interval [CI] 0.63-0.74) and 0.92 (95% CI 0.89–0.94), respectively. Sensitivity ranged across studies from 37% to 90%. Specificity ranged across studies from 78% to 99%. The PLR, NLR, and DOR of the overall analysis of mSEPT9 were 8.1 (95% CI, 5.9-11.2), 0.34 (95% CI, 0.28-0.40), and 24 (95% CI, 16-37), respectively. The summary area under the receiver operating curve (AUC) was 0.89 (95% CI 0.86–0.91).
The authors reported that “Using the meta-regression method, they found that mSEPT9 had a higher, but not statistically significantly different, diagnostic sensitivity and specificity than FIT/FOBT, with p-values of 0.54 and 0.51, respectively.” The sensitivity of FIT/FOBT was 0.59 (95% CI 0.48-0.70) and the specificity was 0.88 (95% CI 0.81-0.96). This suggests that mSEPT9 has a higher but not statistically significant diagnostic value for CRC compared with FIT/FOBT.
Subgroup and meta-regression analyses demonstrated that the diagnostic sensitivity value was statistically significantly higher for Asian ethnicity compared to white ethnicity (p = 0.04). The results showed a statistically significantly higher sensitivity for mSEPT9 test combined with fecal occult blood test (FOBT) or fecal immunochemical test (FIT) than for the mSEPT9 test alone (p =0.01), but there was no difference in specificity (p = 0.24). The diagnostic sensitivity value was statistically significantly higher for the Epi proColon® 2.0 (sensitivity = 0.74) assay than for the other test methods, including Epi proColon® test 1.0 (sensitivity = 0.68, p < 0.01) or RT-PCR (sensitivity = 0.60, p = 0.02). There was no statistically significant differences in specificity between Epi proColon® 2.0 and the other test methods (Epi proColon® 1.0, p = 0.15) and RT-PCR (p = 0.43).
The rate of mSEPT9 positivity was higher in advanced CRC cases compared with early-stage CRC cases, and was higher in CRC cases than in adenoma cases. The mSEPT9 positivity rate was much higher in advanced-stage cases of CRC than in early-stage cases (summary odds ratio [OR] = 0.79, 95% CI 0.66-0.94, p = 0.010). The authors did not define the categories for early versus advanced stage cancers.
The authors acknowledged several limitations as follows: “First, some included studies did not provide the cut-off points when analyzing the diagnostic values; thus, the authors could not exclude the different cut-off points that might significantly influence the diagnostic values. Second, the controls of some of the studies were different, with some using non-CRC patients, some using healthy persons, and others using both. Although they divided the included studies into non-CRC diseases and healthy controls, they could not further divide them into specific colorectal diseases. Third, there was significant heterogeneity across the studies in terms of sensitivity and specificity, which might undermine the reliability of the results. Fourth, this meta-analysis only selected English and Chinese articles; the exclusion of other languages might induce [selection] bias. Fifth, the included studies did not account for the effects of risk factors for CRC, such as age, sex, smoking, diet, and genetic factors on their findings, which may undermine the robustness of the results.”
The authors concluded that “plasma mSEPT9 has a high diagnostic value for CRC, especially with the newly developed Epi proColon® test 2.0 method. The diagnostic sensitivity is superior among Asians compared to whites, and the combination of mSEPT9 and FOBT/FIT demonstrated a better performance than mSEPT9 alone. The expression of mSEPT9 is associated with CRC stage but not with location.”
Song L, Jia J, Peng X, et al. The performance of the SEPT9 gene methylation assay and a comparison with other CRC screening tests: A meta-analysis. Sci Rep. 2017 Jun 8;7(1):3032.
The aim of the study was to review the SEPT9 assay performance and compare it with other in vitro diagnostic (IVD) colorectal (CRC) screening tests. The objective of the study selection is to identify the studies that are clinical studies evaluating the performance of the SEPT9 assay using blood samples from human subjects. The authors searched Ovid MEDLINE, EMBASE, CBMdisc and CJFD database, and identified 25 out of 180 publications screened that reported on the SEPT9 assay performance. Search terms included SEPT9 or septin 9, and colorectal cancer or colorectal carcinoma. Exclusion criteria included letters, reviews, meta-analyses, non-clinical studies, studies not related to mSEPT9 detection assays, not plasma or serum studies, not methylation studies and studies that did not include a statistically significant number of CRC or non-CRC cases.
The authors reported that “In the 25 reports, 22 of them were cohort or case-control studies, while the PRospective Evaluation of SEPTin 9 (PRESEPT) study is the only one carried out so far in the screening background in average-risk population (Potter, 2014) and the PRESEPT study and a recent report by Song et al. performed the opportunistic screening in high-risk population (Song, 2016; Wu, 2016).” The PRESEPT study was comprised of asymptomatic individuals ≥50 years old scheduled to undergo screening colonoscopy at U.S. and German clinical centers and who voluntarily gave blood plasma samples before colon preparation. The studies by Song et al. 2016 and Wu et al. 2016, included samples drawn from a convenience sample of higher risk patients from three hospitals in China that met eligibility criteria. After all planned tests were completed, patients were divided based on clinical status groups according to colonoscopy diagnosis and pathology: CRC, adenoma, proliferative polyps, non-CRC GI diseases (including, inflammatory bowel diseases, colitis, ulcer, abscess, etc.), non-CRC cancers, and NEDs.
The meta-analysis included 2613 CRC cases and 6030 controls, and sensitivity and specificity were used to evaluate its performance at various algorithms. The assay kits included Epi proColon® 1.0 and 2.0, the SensiColon test, the ARUP laboratory developed test (LDT) assay, and different research kits. The SensiColon assay for blood samples was approved by the Chinese FDA (Song, 2016), but not by the US FDA, as of January 21, 2020.
The authors reported that “All studies were divided into four subgroups based on the algorithm used in the interpretation of multiple qRT-PCR (polymerase chain reaction) or high-resolution melting (HRM) data. If the final positive test result was determined from at least one positive count out of three repeats, the study was categorized into the 1/3 algorithm group, and if the final positive test result was determined from at least two positive counts out of three repeats, the study was categorized into the 2/3 algorithm group. Similarly, if the final positive test result was determined from at least one positive count out of two repeats, the study was categorized into the 1/2 algorithm group, while if the final positive test result was determined from only one reaction, the study was categorized into the 1/1 algorithm group.”
The authors reported that “The overall bias of the included studies was tested using the Deeks’ funnel plot, and the P value of 0.77 indicates that the distribution of studies is symmetric and there is no systematic bias across all studies analyzed in this study.” The data showed high I2 values (69.3% to 92.6%) with very small P values, indicating the existence of heterogeneity in studies for all four algorithms. No demographic data was shown.
Overall, the results showed that the sensitivity of these studies ranged from 48.2% to 95.6%, and the specificity ranged from 79.1% to 99.1%. The Epi proColon® 2.0, exhibited a higher sensitivity at 68.2% to 95.6%, and maintained high specificity at 80.0% to 99%.
The publication stated that “In order to compare the performance of SEPT9 assay at various algorithms, the results showed that the 1/3 algorithm exhibited the best sensitivity (0.78) with lowest specificity (0.84) among all algorithms, while 2/3 algorithm exhibited the highest specificity (0.96). The sensitivity and specificity of 2/3 and 1/1 algorithm were very similar exhibiting the best balance between sensitivity and specificity (sensitivity: 0.73 vs 0.74, specificity: 0.96 vs 0.94). The 1/2 algorithm exhibited the lowest sensitivity (0.59) with satisfactory specificity (0.91).” The overall detection rate for stage I and II achieved 59.6% and 85.7%, respectively. The publication reported that the “SEPT9 assay generally exhibited the highest detection rate for all stages of CRC with 1/3 algorithm compared to the other assays.”
The performance of the blood SEPT9 assay in asymptomatic population screening appeared to be lower than that of the FIT and FIT-DNA tests. The authors stated that “…the SEPT9 exhibited lower sensitivity (68.0% for the SEPT9 assay, compared with 79.0% for FIT and 92.3% for FIT-DNA test) and lower specificity (80.0% for the SEPT9 assay, compared with 94.0% for FIT and 86.6% for FIT-DNA test) than FIT or FIT-DNA test.” In a population with symptoms, “the SEPT9 assay exhibited significantly higher sensitivity than the FIT test (75.6% vs 67.1%, p < 0.05), while they showed essentially identical specificity. It appeared that the performance of the SEPT9 assay in screening of symptomatic population is better than that of the FIT test.”
The authors acknowledged several limitations. The study settings differed across the studies. Another limitation is that the reaction system in different studies varied by the volume used, and “this might explain why 1/1 algorithms exhibited higher performance than 1/2 algorithms. The PCR reaction from Epi proColon® series product used 30 μl reaction system…while the latest SensiColon product used 60 μl reaction system with double the amount of DNA template. This allowed a higher chance of methylated DNA detection, although only one PCR reaction was performed.” Another limitation is that given the application of different algorithms determining when the test result was positive, sensitivity and specificity varied with different methods of interpretation of test positivity.
The authors concluded that the performance of the blood SEPT9 assay appeared to be less potent than FIT and multitargeted stool DNA (FIT-DNA) tests in an asymptomatic population but was superior to that of the serum protein markers and the fecal immunochemical test (FIT) test in a population with symptoms. They concluded that the 1/3 algorithm that has a high sensitivity is recommended for CRC screening, while the 2/3 or 1/1 algorithms with a high specificity are suitable for early detection of CRC for diagnostic purposes to exclude healthy subjects. The SEPT9 assay exhibited better performance
in symptomatic population than in a population without symptoms.
Yan S, Liu Z, Yu S, et al. Diagnostic Value of Methylated Septin9 for Colorectal Cancer Screening: A Meta-Analysis. Med Sci Monit. 2016 Sep 25;22:3409-3418.
The aim of the study was to determine the diagnostic accuracy of methylated Septin9 (mSEPT9) for colorectal cancer (CRC) and to evaluate its diagnostic utility compared to FOBT in CRC patients. They compared the Epi proColon® test with the non-Epi proColon® test for mSEPT9 detection by performing a meta-analysis. The authors reported that “Studies published in English were carefully searched in biological databases (PubMed, Embase, EBSCO, Web of Science, Science Direct, and Cochrane Library) up to September 2015. The search terms were as follows: (Colorectal cancer, Colorectal carcinoma, or CRC) AND (SEPT9 gene methylation, Methylated SEPT9 DNA, methylated Septin9 or mSEPT9). Studies eligible for inclusion met the following criteria: i) articles that investigated the association between mSEPT9 DNA expression levels and CRC diagnosis using a clearly defined test method; ii) articles that measured the expression of mSEPT9 in plasma or serum; iii) articles published as full-text paper in English; and iv) sensitivity and specificity of mSEPT9 were obtained from the text. Studies for exclusion met the following criteria: i) abstracts, letters, and reviews; ii) non-English-language papers; iii) articles reported mSEPT9 RNA or protein only; iv) laboratory studies; v) articles contained insufficient data for calculating sensitivity and specificity; vi) samples came from tissues or other body fluids; and vii) unknown detection methods.” Publications were also excluded for each of the following reasons: Performance of SEPT9 in prognosis of CRC (n=1), no control group (n=1), and great heterogeneity (n=1). The authors stated that “After reviewing relevant studies, accuracy measures (pooled sensitivity and specificity, positive/negative likelihood ratio [PLR/NLR], and diagnostic odds ratio [DOR]) were calculated for mSEPT9 in the diagnosis of CRC. Overall test performance was summarized using summary receiver operating characteristic curve analysis” to calculate the area under the curve (AUC).
A total of 14 studies were recruited, which consisted of one cohort study and 13 case-control studies. The authors reported that “There were 9870 subjects in total and the numbers of CRC patients, non-CRC patients (adenoma, polyp, and benign diseases), and healthy subjects were 1205, 3735, and 4930, respectively. All patients with CRC were diagnosed based on pathological confirmation” of CRC. No sociodemographic data was shown. No overall measure of study heterogeneity, such as the I2 statistic was shown for the overall study.
For the test methods, seven studies used the Epi proColon® test and seven used a reverse transcription polymerase chain reaction (RT-PCR) test. However, two studies were misclassified as using an RT-PCR test and not the Epi proColon® test when, in fact, the studies (Jin, 2015; Johnson, 2014) actually used the Epi proColon® test. The other five studies (He, 2010; Lee, 2013; Lofton-Day, 2008; Tham, 2014; Toth, 2014) used an RT-PCR test, which were research kits, and not FDA approved.
For the results, pooled sensitivity and specificity, and corresponding 95% confidence intervals (CI), of mSEPT9 for CRC diagnosis were 0.66 (95% CI: 0.64–0.69) and 0.91 (95% CI: 0.90–0.91). Sensitivity of the mSEPT9 test ranged from 36.6% to 90%. Specificity ranged from 69% to 98.9%. For PLR, NLR, and DOR, the pooled values were 5.59 (95% CI: 4.03–7.74), 0.37 (95% CI: 0.29–0.48), and 16.79 (95% CI: 10.54–26.76), respectively. The area under the summary ROC (receiver operating characteristic) curve (AUC) was 0.856. The pooled sensitivity and specificity for Epi proColon® test in a subgroup analysis were 0.63 (95% CI: 0.58–0.67) and 0.91 (95% CI: 0.90–0.92), respectively. The publication also stated that “The AUCs in the Epi proColon® test and non-Epi proColon® test for CRC diagnosis were 0.871 and 0.797, respectively. In head-to-head comparison of diagnostic accuracy of SEPT9 compared to FOBT, AUC of mSEPT9 and FOBT for CRC diagnosis were 0.786 and 0.657, respectively.” The sensitivity of mSEPT9 was 76% compared to 67% for FOBT. The specificity of mSEPT9 was 87% compared 91% for FOBT.
The authors acknowledged some potential study limitations. First, it was impossible to determine the sources of heterogeneity due to the small number of studies, and the presence of clinical heterogeneity in the study may have affected the generalizability of the results. Second, this meta-analysis mostly included case-control studies, which may be prone to selection bias because controls are selected based on not having the target condition. In addition, there are only three well-designed head-to-head comparisons in the studies.
The authors concluded that the present study demonstrated that mSEPT9 can be a good diagnostic biomarker complementary to FOBT because mSEPT9 has superior sensitivity compared to FOBT. In the head-to-head comparison of mSEPT9 and FOBT for the diagnosis of CRC, the AUC showed that mSEPT9 had a higher diagnostic efficiency compared to FOBT. The AUC of the Epi proColon® test was higher than that of the non-Epi proColon® test, suggesting that the Epi proColon® test was better for the diagnosis of CRC by mSEPT9.
Comparison Studies
Church TR, Wandell M, Lofton-Day C, et al.; PRESEPT Clinical Study Steering Committee, Investigators and Study Team. Prospective evaluation of methylated SEPT9 in plasma for detection of asymptomatic colorectal cancer. Gut. 2014 Feb;63(2):317-25.
The aim of the PRospective Evaluation of SEPTin 9 (PRESEPT) study was to estimate the accuracy of circulating methylated SEPT9 DNA (mSEPT9) to detect invasive colorectal cancer (CRC) in patients meeting average risk screening guidelines in the context of routine screening. The prospective study had a study population comprised of asymptomatic individuals ≥50 years old scheduled to undergo screening colonoscopy at 32 US (22) and German (10) clinical centers and who voluntarily gave blood plasma samples before colon preparation. To identify individuals considered to be of average risk, the study “excluded those with previous lower endoscopy, previous CRC or adenomas; iron deficiency anaemia or haematochezia (blood in the stool) within the previous 6 months; or family history indicating increased risk for the disease (two or more first degree relatives with CRC or one or more with CRC at age 50 years or less; or known Lynch syndrome or familial adenomatous polyposis). To increase accrual, approximately 6 months after study initiation the Clinical Studies Steering Committee (CSSC) revised the initial eligibility criteria to no longer exclude subjects with flexible sigmoidoscopy more than 5 years before enrollment.”
Using a commercially available assay, the first generation Epi proColon® Assay (Epigenomics AG, Berlin, Germany), three independent blinded laboratories assayed plasma DNA of all CRC cases and a stratified random sample of other subjects in duplicate real time polymerase chain reactions (PCRs) using two separate PCR replicates. If at least one PCR replicate from a subject was positive, the assay was positive. The authors stated that “Based on review of the clinical and histopathological characteristics documented on study data forms, the CSSC, prior to assay, assigned each adequate colonoscopy outcome (those with adequate preparation and complete to the caecum) to one of four clinical classes: CRC, advanced (clinically significant) adenomas (AA), non-advanced (clinically insignificant) adenomas (NA), or no evidence of disease (NED).”
The authors also clarified that “In order to analyze the effect of a different and possibly improved analysis method, a single post hoc study examined the impact of an additional PCR replicate (i.e., three rather than two wells per subject) on sensitivity and specificity…As the post hoc study was done in response to initial results from the main study indicating lower than expected sensitivity of the original assay, it is an exploratory analysis and, unlike the main study result, cannot be considered a validation.”
The study population consisted of 7941 men (45%) and women (55%), who had a mean age 60 years enrolled from June 2008 until January 2010. The authors reported that “Among the 53 cancer cases, 66% were men and mean age was 67 years; among the non-CRC subjects, 45% were men and mean age was 61 years.”
For the results among the 53 CRC cases and 1457 subjects without CRC, the sensitivity of mSEPT9 for detecting colorectal cancer was 48.2% (95% confidence interval [CI] 32.4% to 63.6%; crude rate 50.9%). For staged CRC, the sensitivity was 35.0% for stage I, 63.0% for stage II, 46.0% for stage III, and 77.4% for stage IV. Specificity was 91.5% (95% CI 89.7% to 93.1%; crude rate 91.4%). Advanced (clinically significant) adenomas (AA) had a low sensitivity (11.2%). The authors also reported “…the assay showed greater sensitivity and specificity in younger subjects (<65 years of age) than in older ones, but the differences were not statistically significant.”
The authors acknowledged several limitations to their study: “Because the centers enrolling in the study were not randomly sampled and study subjects were sampled from the study centers disproportionately by clinical findings for laboratory testing, standardization to a target screening population was necessary to obtain relevant performance estimates. Although in any non-random sample there may be unknown factors for which standardization is impossible and there is always some error in the standardization variables, their standardization included the main determinants of CRC incidence, age and sex, and they had negligible measurement errors.” Another limitation was that to increase accrual, the entry criterion regarding prior endoscopy was relaxed soon after the beginning of enrollment. This probably reduced the overall prevalence rate, but the authors believed it had little impact on the assay parameter estimation. A potential limitation was that “no split sample quality control was performed to examine consistency between laboratories, but there was no statistically significant difference in the frequency of findings between them (data not shown).” Another potential limitation was that “although subjects with other cancers found on examination were excluded from the primary analysis, sensitivity analyses including these cases only slightly affected the quantitative results (analyses not shown).”
The authors also acknowledged another limitation in that “tissue samples from the current study were not collected for testing to determine whether the tumor sample contained significant amounts of mSEPT9.” Another limitation the authors reported was with the post hoc analysis (results not included in this NCD summary): “this post hoc analysis imprecisely reproduced a simultaneous three replicate assay, for three reasons: (1) the decision to look at a third PCR replicate was based on lower than expected two replicate assay sensitivity, leading to lower estimated three replicate assay sensitivity; (2) the third PCR replicates were not done in the same run on the same machine as the first two, unlike an actual three PCR replicate assay, allowing increased run to run variation to lower the assay discrimination; and (3) criteria for invalid results differ slightly because in practice, all three replicates would have common control samples and be subject to the same probability of invalidity. For these reasons, estimated sensitivity of the three replicate assay is likely to be smaller than true sensitivity; the effect on specificity is less clear but probably small. Thus, the three replicate results are strictly exploratory. In addition, because the assay is working with what are small quantities, the assay involves a stochastic component, and hence a particular PCR replicate may lack adequate numbers of mSEPT9 copies to trigger DNA amplification. Additional replicates merely provide more opportunities to yield a positive, thus increasing sensitivity while decreasing specificity. Therefore, it can only be speculated whether this more recent assay version might perform better in the screening setting.”
The authors concluded that the blood-based mSEPT9 test showed that a CRC signal in blood can be detected in asymptomatic average risk individuals undergoing screening. Although the results render the clinical utility to be very low, the authors suggested that there might be ways to achieve possible improvements, as suggested by in their post hoc analysis. However, the utility of the test for population screening for CRC will require improved sensitivity for detection of early cancers and advanced adenomas. Further, blood-based tests have long been sought in the cancer detection field for their convenience and potential for higher compliance; nevertheless, higher uptake, higher yield of precancerous lesions and finally any effect on mortality would still have to be shown.
He N, Song L, Kang Q, et al. The Pathological Features of Colorectal Cancer Determine the Detection Performance on Blood ctDNA. Technol Cancer Res Treat. 2018 Jan 1;17:1533033818791794.
The study aim was “to investigate the significance of the clinicopathological factors on methylated SEPT9 performance in a symptomatic endoscopy cohort, with a specific focus on colorectal cancer.” The study recruited 1160 participants from 3 Chinese hospitals; of these, 300 patients had colorectal cancer, 122 patients had adenoma, 103 patients had hyperplastic polyps, 568 had no evidence of disease (NED), and 67 patients had other gastrointestinal diseases. Investigators also collected peripheral blood samples from all participants before colonoscopy and measured the methylated SEPT9 level using the Epi proColon® 2.0 assay. Among the CRC group, 55.3% were at least 60 years old and 49.3% were women. Among all patients (including CRC), 31.9% were at least 60 years old and 43.7% were women.
For the results, sensitivity or positive detection rate (PDR) for CRC, adenoma, other gastrointestinal disease (GID), hyperplastic polyps (HP), and NED groups was 73.7%, 27.0%, 16.4%, 8.7%, and 3.0%, respectively. The authors reported that “…All examined diseases, including HP (X2= 7.73, P < .01), other GID (X2= 25.63, P < .001), adenoma (X2= 86.47, P < .001), and all stages of CRC (X2 = 492.71, P < .001) exhibited statistically significantly higher PDR than that of the NED group… If CRC was defined as the positive group, and NED was defined as the negative group, the sensitivity was 73.7% (221/300), and the specificity was 97.0% (551/568).” The authors also reported that “Cancer stage, size, and invasion depth were positively correlated with the detection sensitivity, while no difference in sensitivity was identified among cancers at various locations” within the colon. For instance, “the PDR for stage 0, I, II, III, and IV CRC was 60.9%, 54.8%, 80.8%, 75.0%, and 91.7%, respectively. Stage II, III, and IV showed statistically significantly higher sensitivity than stage 0 and I (X2 = 11.99, P < .001).” The authors did not acknowledge any limitations.
The authors concluded that “factors that reflect the colorectal cancer intrinsic properties, including cancer stage, size, invasion depth, classification, differentiation, and metastasis, exhibited a significant effect on the mSEPT9 detection performance.” Their observations suggest that SEPT9 methylation could be a marker to assess CRC progression or prognosis, and to establish therapeutic strategies.
Hitchins MP, Vogelaar IP, Brennan K, et al. Methylated SEPTIN9 plasma test for colorectal cancer detection may be applicable to Lynch syndrome. BMJ Open Gastroenterol. 2019 May 28;6(1):e000299.
The aim of the exploratory retrospective case control study was to assess the utility of mSEPT9 for CRC detection in high-risk patients with Lynch syndrome (LS). The authors reported that “All patients included in this study had confirmed LS, as defined by carriage of a pathogenic germline mutation within one of the DNA mismatch repair (MMR) genes.” The publication reported on two investigations to measure mSEPT9 in patients with LS based on samples obtained from two different (but minimally overlapping) time periods. That testing involved: pyrosequencing to assess archived tissue samples and a modified version of the Epi proColon® 2.0 CE mSEPT9 test to plasma samples.
The first investigation used archived tissue samples to assess whether Lynch-associated colorectal neoplasia produced an mSEPT9 biomarker. Archived tissue specimens were available from patients with invasive CRC, patients with advanced adenomas, and patients with macroscopically normal colorectal mucosa (NCM). The authors reported that the patients “underwent either surgical resection for a diagnosis of CRC or a polypectomy during colonoscopy (CL) between December 1982 and December 2009. The specimens had been archived in formalin-fixed paraffin-embedded (FFPE) tissue blocks.” To incorporate hypermethylated and unmethylated controls, the investigators used DNA from the RKO CRC cell line and PBL from a healthy control, respectively. The study measured SEPT9 methylation in bisulfite-converted DNA using CpG pyrosequencing. The investigators calculated methylation values as the mean percentage methylation across the five CpG sites.
For the investigation of plasma samples, peripheral blood was drawn for patients with LS by venipuncture between March 2006 and February 2019. The authors reported that the “LS case groups included 20 peri-surgical cases with a colonoscopy-based diagnosis of CRC (stages I-IV), 13 post-surgical metastatic CRC cases, and 17 pre-diagnosis cases. The control group comprised 31 cancer-free LS subjects.” The study site was not identified.
The authors explained that “To detect mSEPT9 as circulating tumor DNA, the plasma-based mSEPT9 test was retrospectively evaluated in plasma samples from LS subjects with and without a CRC diagnosis using the Epi proColon® 2.0 CE Assay adapted from 1 ml plasma using the 1/1 algorithm.” All the patients with CRC had colonoscopy-based diagnosis: (1) blood drawn preoperatively or perioperatively; (2) blood drawn up to 1 year prior to the colonoscopy procedure (3) cases “diagnosed with metastatic CRC during postoperative surveillance for relapse.” As previously stated, “plasmas from LS subjects without a prior diagnosis of cancer or preneoplastic lesions, and who did not go on to develop cancer within 2 years after the blood draw were included as controls.”
For the tissue specimens, in the CRC group, the mean age at diagnosis was 55.3 years (± 15.6 years) and 72.2% were men. For the result, an analysis of the distribution and methylation levels across the entire SEPT9 gene in CRC and NCM (control) tissues found that the V2 region “had the most frequent and the highest levels of differential methylation between CRC and NCM tissues.” The investigators pointed out that this is the same region targeted by the plasma-based Epi proColon® 2.0 CE test. The authors also reported that “the assay had a limit of detection down to 2.5% (coefficient of variance of 0.07), and strong linearity with methylation levels (r2>0.975). They further reported that “the mSEPT9 biomarker is similarly frequent in Lynch-associated CRC (97%) as in sporadic CRC (96%), and is also found in 90% of advanced adenomas of various histologies.”
For the plasma samples, the mean age of the CRC group at the time of the blood draw was 48 years; the publication did not present the proportion that were male. The authors reported that “sensitivity of plasma mSEPT9 to detect CRC (stages I-IV) around the usual time of diagnosis was 70.0% (95% CI, 48%-88%) [in Lynch Syndrome cases] with a colonoscopy-based CRC diagnosis and 92.3% (95% CI, 64%-100%) in post-surgical metastatic cases. Specificity in cancer free controls was 100% (95% CI 89%-100%). In pre-diagnosis cases, plasma mSEPT9 was detected within two months prior to colonoscopy-based CRC diagnosis in 3/5 [60%] cases.”
The authors acknowledged several study limitations: “First, the sample size available for study within each group of CRC cases and the cancer-free controls was too small for precise estimates of sensitivity and specificity, and plasma was not available from LS subjects with advanced PCL. A second limitation was that only 1 mL plasma was available for testing, which may have led to an underestimation of sensitivity, and an overestimation of specificity, of mSEPT9 to detect CRC.” They argue that sensitivity for any liquid biopsy-based test to detect CRC is more important than specificity in the context of high-risk groups.
The authors concluded that their preliminary findings suggest that the plasma-based mSEPT9 test might be applicable for CRC screening in subjects with Lynch Syndrome. The mSEPT9 test may demonstrate similar diagnostic performance characteristics in Lynch Syndrome as in the average-risk population.
Jin P, Kang Q, Wang X, et al. Performance of a second-generation methylated SEPT9 test in detecting colorectal neoplasm. J Gastroenterol Hepatol. 2015 May;30(5):830-3.
The aim of the retrospective case-control study was to evaluate the efficacy of the second-generation SEPT9 assay for the detection of colorectal neoplasm in a Chinese population, and to compare it with fecal immunochemical test (FIT). Peripheral blood samples were taken from 6298 patients seen in the Beijing Military General Hospital Endoscopy Center between March 2013 and April 2014 before colonoscopy preparation. The authors reported that “Patients with known inflammatory bowel disease, Lynch syndrome, familial adenomatous polyposis, Peutz-Jeghers syndrome, or other malignant diseases were excluded. Adenomatous polyps with > 25% villous component, high-grade dysplasia (HGD), or diameter ≥ 10 mm were considered as advanced adenomas...A total of 135 patients with CRC, 169 with adenomatous polyps, 81 with hyperplastic polyps, and 91 healthy controls were included…The clinical status of all subjects was verified by colonoscopy…None of the patients received chemotherapy, radiotherapy, endoscopic, or surgical intervention before colonoscopy.” Plasma was isolated from the blood samples from 476 patients that ultimately comprised the study population. The plasma samples were tested for SEPT9 testing using Epi proColon® 2.0 test. Of the 476 patients, fecal samples were available for 177 patients prior to colonoscopy testing. In these 177 patients, both SEPT9 and FIT were performed. Among the 135 CRC patients, the mean age was 60.9 years (± 12.1 years, range 28-84 years) and 51.1% were women.
For the results, “the sensitivity and specificity of SEPT9 for CRC were 74.8% (95% confidence interval [CI]: 67.0–81.6%) and 87.4% (vs non-CRC, 95% CI: 83.5–90.6%), respectively. SEPT9 was positive in 66.7% of stage I, 82.6% of stage II, 84.1% of stage III, and 100% of stage IV CRCs. The sensitivity of SEPT9 for advanced adenomas was 27.4% (95% CI: 18.7–37.6%). The sensitivity and specificity of FIT for CRC was 58.0% (95% CI: 46.1–69.2%) and 82.4% (95% CI: 74.4–88.7%), respectively…SEPT9 detected 25 cancers that were missed by FIT, whereas FIT detected 12 cancers that were missed by SEPT9. The difference in discordant test results was statistically significant (p = 0.033). In a post-hoc analysis among CRC without metastasis (stage I–III), the sensitivity of SEPT9 was statistically superior to that of FIT (76.4% vs 56.4%, p = 0.041).”
The authors acknowledged several limitations: “First, it was a retrospective case–control study, and the subjects were not all asymptomatic average-risk persons. So the performance estimates may differ substantially in prospective screening setting in which the test would be applied. Second, though [they] compared test performance between the SEPT9 assay and FIT, some important parameters such as patient compliance or cost-effectiveness could not be assessed.”
The authors concluded that SEPT9 showed better performance in CRC detection than FIT, but similar for advanced adenomas. With improved performance characteristics in detecting CRC, the second generation SEPT9 assay could play an important role in CRC screening and early detection.
Johnson DA, Barclay RL, Mergener K, et al. Plasma Septin9 versus fecal immunochemical testing for colorectal cancer screening: a prospective multicenter study. PLoS One. 2014 Jun 5;9(6):e98238.
The aim of the study was to compare the performance of a new Septin9 DNA methylation based blood test, the Epi proColon® test, with a fecal immunochemical test (FIT) for colorectal cancer (CRC) screening, using colonoscopy as the reference standard. This prospective cohort multicenter study was designed to collect matched blood and stool specimens from screening guideline eligible subjects across 61 sites in the United States. Subjects aged 50-84 years were enrolled between March 30, 2012 and November 26, 2012. To compare test sensitivity for CRC, the study population comprised of patients who had been diagnosed with CRC through screening colonoscopy (Group A, n = 102) who were enrolled and provided fecal and blood samples following colonoscopy but prior to resection surgery. To compare test specificity, patients were enrolled prospectively (Group B, n = 199) and provided fecal and blood samples prior to bowel preparation for screening colonoscopy. The authors reported that “Exclusion criteria included a previous history of CRC or previous colonoscopy resulting in recommendation for repeat colonoscopy at an interval less than ten years (high risk population); neoadjuvant treatment; familial history of CRC; history of inflammatory disease; acute or chronic gastritis; current diagnosis of cancer other than CRC; overt rectal bleeding or bleeding hemorrhoids; known infection with HIV, HBV or HCV; and receiving intravenous fluid at the time of the sample collection. Subjects with a curative biopsy during screening colonoscopy were also not included.”
Blood plasma and fecal samples were analyzed using the Epi proColon® and OC Fit-Check tests respectively. Among the 102 diagnosed colorectal cancer patients, 68% were men, 76% were at least 60 years old, and 69% were Caucasian.
For the results, three of the 102 Group A subjects were reclassified as advanced adenomas based on pathology review and 99 subjects had a confirmed diagnosis of CRC. From the Group B subjects, two were diagnosed with CRC for an aggregate across both groups of 101 CRC cases. Of the 101, all had blood samples and 97 had stool samples. Compared to the reference standard colonoscopy, sensitivity for CRC detection using Epi proColon® Septin9 was 73.3% (95% confidence interval [CI] 63.9–80.9%, n = 74/101) and sensitivity using FIT was 68.0% (95% CI 58.2–76.5%, n = 66/97). For paired blood and fecal samples (dropping the results for subjects without stool samples), the sensitivity of the Epi proColon® test (72.2%; 95% CI 62.5–80.1%, n = 70/97) was shown to be statistically non-inferior to FIT (68.0%; 95% CI 58.2–76.5%, n = 66/97).
The investigators estimated specificity from all non-CRC subjects combined across groups A and B, regardless of classification of advanced adenomas, small polyps or no evidence of disease (n =200, 193 of 200 with stool samples). Specificity of the Epi proColon® test was 81.5% (95% CI 75.5–86.3%, n = 37/200) compared with 97.4% (95% CI 94.1–98.9%, n = 5/193) for FIT. Specificity for samples with paired tests was 80.8% (95% CI 74.7%-85.8%, n = 37/193) and 97.4% (95% CI 94.1%-98.9%, n = 5/193)
for Epi proColon® and FIT, respectively, indicating a significantly lower specificity for Epi proColon®.
When test results for Epi proColon® and FIT were combined, CRC detection was 88.7% (n = 86/97) at a specificity of 78.8% (false positives = 41/193 or 21.2%). The authors reported that “When comparing test performance in early stage cancer (0, I, II) there was no significant difference (Mc Nemar test, p-value = 1), with Epi proColon® detecting 34/48 (70.8%) of subjects compared with 33/48 (68.8%) detection with OC FIT-CHEK. Although there were differences in point estimate for stage III and for stage IV observed, these differences were also not significant (Mc Nemar test, p-values = 0.29 and 0.14, respectively). Analysis of test performance based on tumor location (left or right colon) showed no difference for either test, with an observed 73.1% (left) vs 75% (right) for Epi proColon® (n= 88) and 70.6% (left) vs 69.4% (right) for OC FIT-CHEK (n= 87).”
The authors acknowledged several limitations in their study. The study did not compare patient compliance or assess patient preferences. Also this study was not designed to address the cost-effectiveness of Epi proColon® relative to other screening strategies.
The authors concluded that at a sensitivity of 72%, the Epi proColon® test was non-inferior to FIT for CRC detection, although at a lower specificity. With negative predictive values of 99.8%, both methods are identical in confirming the absence of CRC. The Septin9 test did have a higher positivity for subjects who were negative for CRC, and would result in an increased number of follow-up colonoscopies.
Ørntoft MB, Nielsen HJ, Ørntoft TF, et al. Performance of the colorectal cancer screening marker Sept9 is influenced by age, diabetes and arthritis: a nested case-control study. BMC Cancer. 2015 Oct 29;15:819.
The aim of the study was to test the hypothesis that comorbidities and/or demographic characteristics affect the results of the Sept9 test. The retrospective case–control study was nested in a cohort from the prospective Danish Endoscopy II study, a multicenter initiative that compiled a dataset with samples from 4698 patients who have been referred for diagnostic colonoscopy due to colorectal cancer (CRC)-related symptoms in Denmark. Plasma samples were obtained from 150 cancer and 150 controls with no evidence of CRC disease (NED) selected from the Endoscopy II cohort of 4698 subjects. The cases and controls were matched on age and gender, and cases were stratified by tumor-site and tumor-stage. Cases consisted of 35 stage I CRC, 35 stage II CRC, 30 stage III CRC and 29 stage IV CRC based on Union for international cancer control (UICC) criteria. The authors reported that “Exclusion criteria were previous colonoscopy, previous CRC or adenoma, diagnosis with HNPCC (Hereditary Nonpolyposis Colorectal Cancer or Lynch Syndrome) or FAP (Familial adenomatous polyposis), previous or present extracolonic malignant disease, or age under 18. Just prior to colonoscopy all subjects had a blood sample collected.” Plasma methylated Sept9 DNA levels were assessed using a commercially available polymerase chain reaction (PCR) based assay (Epi-proColon®) with PCR performed in triplicate (1/3 and 2/3 refers to the PCR-algorithms affirming a sample as positive if 1 of 3 or 2 of 3 PCR replicates had a valid curve). Interventions followed the Danish Colorectal Cancer Group (DCCG) guidelines. Among the colorectal cancer cases, 42% were above age 65 years and 51% were women.
For the results, the authors reported on findings for the 1/3 algorithm and the 2/3 algorithm. Using the 1/3 algorithm, sensitivity for CRC stages I-IV was 37 % (95% CI, 21-55%), 91% (95% CI, 76-98%), 77% (95% CI 58-90%), and 89% (95% CI 72-98%), and the overall sensitivity 73 % (95 % CI, 64–80 %) and specificity 82 % (95 % CI, 75–88 %), respectively. The sensitivity was significantly lower for stage I than for the higher stage tumors (Wilcoxon rank sum test, p < 0.001).
Using the 2/3 algorithm, sensitivity for CRC stages I-IV was 17 % (95% CI, 7-34%), 74% (95% CI, 57-88%), 63% (95% CI 44-80%), and 86% (95% CI 67-96%), and the overall sensitivity 59 % (95 % CI, 50–67 %) and specificity 95 % (95 % CI, 91–98 %), respectively.
Age >65 was significantly associated with both increased false positive and false negative results (p < 0.05). However, the authors pointed out that finding might be an artifact of an underlying imbalance in tumor stage distribution; subjects in the >65 age group had significantly fewer stage III and IV tumors. Arthritis was associated with a higher false negative rate (p = 0.005) whereas arteriosclerosis was associated with a higher false positive rate (p = 0.007). Diabetes was associated with Sept9 positivity with an OR of 5.2 (95 % CI 1.4–19.1). When the performance of Sept9 was adjusted for these parameters (age, arthritis, arteriosclerosis, and diabetes) in a final multivariate regression model, the odds ratio (OR) for a positive Sept9 test to be associated with CRC increased from 8.25 (95 % CI 4.83–14.09) to 29.46 (95 % CI 12.58–69.02).
The authors acknowledged that one “limitation of the study is the size of the cohort, which counted 299 subjects. Accordingly, near-significant differences between cases and controls (Type II error, [a false negative finding]) may still reflect potentially interesting observations. Another limitation is that the Sept9 test is validated for 3.5 mL of plasma and only 139 subjects fulfilled this requirement. Though no significant difference was observed as a result of the lower plasma volume, this could influence especially the overall assay sensitivity.” The last limitation is that the study “allowed for a wide age range in the cohort with 45 subjects <50 years of age. Therefore the age of the cohort differs slightly from that of a screening cohort, where all subjects were >50. The wide age range may enhance the differences in assay performance due to age when subjects >65 are compared to subjects ≤65.”
The authors concluded that “the performance of the Sept9 assay was negatively affected by several factors commonly associated with CRC screening populations: early-stage disease, age > 65 years, diabetes, arthritis, and arteriosclerosis. This should be taken into account if the Sept9 assay is used as a single marker for CRC screening, but may also have a wider impact, as it is likely that such factors may affect other blood-based DNA markers as well.”
Potter NT, Hurban P, White MN, et al. Validation of a real-time PCR-based qualitative assay for the detection of methylated SEPT9 DNA in human plasma. Clin Chem. 2014 Sep;60(9):1183-91.
The aim of the retrospective comparative study was to describe the analytical characteristics of the test for detecting methylated SEPT9 DNA in blood and its clinical validation by use of samples from subjects enrolled in the prospective PRESEPT clinical trial conducted in the US and in Germany. Clinical performance was evaluated in a retrospective study by use of samples (n = 1544) from subjects enrolled in the PRESEPT prospective clinical trial. This was assessed using archived prospectively collected plasma samples from the PRESEPT clinical trial (NCT00855348). The authors reported that “PRESEPT enrolled a total of 7941 participants, of whom 6857 fulfilled all study criteria. Though derived from the PRESEPT cohort, the samples used in this study were selected without knowledge of their SEPT9 test outcome in the PRESEPT study and were tested independently from the PRESEPT study. Available participant samples included 50 with invasive adenocarcinoma (CRC), 653 with advanced adenoma (AA), 2369 with small polyps (SP), and 3785 with no evidence of disease (NED). In this study, all available samples from participants with CRC and AA were tested. As PRESEPT included both US and non-US sites, a stratified random selection of the SP and NED groups was performed to enable an assessment of the impact of demographic parameters (sex, age, ethnicity, country of origin) of the US population” on the study results. “Subjects with colorectal cancer were classified as such and grouped further on the basis of stage (I, II, III, or IV)…Subjects with no lesions in screening colonoscopies were classified as no evidence of disease (NED).” Results were analyzed by comparison with colonoscopy, the reference standard.
The samples were processed using Epi proColon® test kits. The authors explained that “Participant samples were called SEPT9 positive if at least 1 methylated SEPT9 Ct value was reported by the instrument software…Samples were called negative if no methylated SEPT9 Ct was reported in any of the 3 valid PCR replicates.” In the final sample set, 60% were above age 60 years, 47% were women, and 73% White, with 81% from the U.S. and 19% from Germany.
The analytical results showed that the limit of detection (LoD) for all samples was 7.8 pg/mL (95% CI 5.8 –10.4 pg/mL) or approximately 1.2 genome equivalents of methylated SEPT9 per milliliter. For reproducibility, the overall percentage agreement estimated to be 94.4% (95% CI 90.7%–96.7%).
The clinical results showed that the sensitivity for all stages of CRC was 68% (95% CI 53%–80%) and for stage I–III CRC, 64% (95% CI 48%–77%). The sensitivity for Stage I colorectal cancer was 41% (95% CI 22-64%), Stage II 83% (95% CI 55-95%), Stage III 80% (95% CI 49-94%) and Stage IV 100% (95% CI 57-100%). Specificity, on the basis of negative colonoscopy findings, was 80.0% (95% CI 78%–82%), when adjusted to the PRESEPT cohort.
The authors acknowledged a limitation in that for patients with a positive SEPT9 test, the proportion with CRC is increased compared with the untested population for a positive predictive value (PPV) of 2.5%. Although this is lower than the PPV for FIT (8.4%), the authors state that this difference needs to be weighed against the potential value that a simple blood-based test can offer toward increasing CRC screening participation, as an alternative method for patients struggling with current screening options. Regardless, because of the low prevalence of CRC, the PPV for any CRC screening test is relatively low.
The authors concluded that the Epi proColon® test was a simple, real time PCR–based assay for the detection of methylated SEPT9 DNA in blood that may provide a noninvasive CRC screening alternative for people noncompliant with current CRC screening guidelines.
Song L, Peng X, Li Y, et al. The SEPT9 gene methylation assay is capable of detecting colorectal adenoma in opportunistic screening. Epigenomics. 2017 May;9(5):599-610.
The aim of the comparative study was to validate the detection of precancerous colorectal adenoma in opportunistic screening using the SEPT9 gene methylation assay. Although the study design was not identified, the investigators collected blood samples from a convenience sample of higher risk patients that met eligibility criteria prior to determining clinical status through colonoscopy and subsequent pathology at three hospitals in China. The investigators collected plasma samples from a total of 1361 subjects, including 85 with colorectal cancer, 364 with adenomas, 216 hyperplastic polyps, 372 other gastrointestinal diseases and 324 normal subjects with no evidence of disease (NED). The authors reported that “Patients with adenoma were grouped into serrated, tubular, tubulovillous and villous adenoma groups based on the results from pathological examinations...None of the subjects received chemotherapy, radiotherapy or surgical intervention before the blood draw and the colonoscopy examination.”
The samples were tested using the Epi proColon® 2.0 CE assay. The authors assessed the performance of the SEPT9 assay for detecting various colorectal diseases with 1/3, 2/3 or 3/3 algorithms (meaning that a sample was overall considered positive if the indicated proportion of the three PCR replicates yielded a positive result). However, the authors clarified that they used the 1/3 algorithm for data interpretation in this study because: 1) it provides highest sensitivity for adenoma and early CRC detection, 2) the sensitivity for all disease groups, except polyps, exhibited significant differences to that of the normal control (NED), and 3) further examinations, such as colonoscopy, can be performed to exclude false positive subjects from CRC or precancerous diseases.
No demographic data was shown.
For the results, the SEPT9 assay using the 1/3 algorithm detected 38.7% of all types of adenoma which was significantly higher than that of the NED group (17.9%, χ2 = 36.20; p < 0.001). When categorized by adenoma subgroup, the assay detected 27.8% of serrated adenoma, 28.7% of tubular adenoma, 53.7% of tubulovillous adenoma and 83.3% of villous adenoma. It also detected 27.5% of nonadvanced adenoma (NAA), 47.0% of advanced adenoma (AA) without high-grade dysplasia and 62.5% of AA with high-grade dysplasia. The average adenoma detection rate was 31.8% (95% CI: 28.3–35.4%). The overall positive detection rate (PDR) for CRC was 87.1%. The PDR for stage I, II, III and IV at 77.8%, 78.9%, 96.8% and 100.0%, respectively. Using the 2/3 algorithm, the overall PDR for CRC was 81.2%. The PDR for stage I, II, III and IV at 66.7%, 73.7%, 90.3% and 100.0%, respectively. Using the 3/3 algorithm, the overall PDR for CRC was 64.7%. The PDR for stage I, II, III and IV at 64.7%, 33.3%, 80.6% and 100.0%, respectively. The authors did not acknowledge any limitations.
The authors concluded that their study provides evidence that in the screening setting, the SEPT9 assay is effective in the detection of advanced adenoma, which is a widely recognized precancerous lesion for CRC. The detection of early-stage CRC in this setting maintained a high sensitivity. Thus, the high sensitivity for advanced adenoma and early stage CRC supports the use of the SEPT9 assay for screening of both precancerous advanced adenoma and CRC in an opportunistic screening setting.
Song L, Jia J, Yu H, et al. The performance of the mSEPT9 assay is influenced by algorithm, cancer stage and age, but not sex and cancer location. J Cancer Res Clin Oncol. 2017 Jun;143(6):1093-1101.
The aim of the comparative study was to examine the influence of algorithm and subject-related factors, including cancer stage, age, sex, and cancer location, on the performance of the SEPT9 gene methylation test. A total of 1225 subjects were recruited in this opportunistic screening study from three Chinese hospitals, including 388 CRC patients, 139 subjects with adenoma, 108 subjects with hyperplastic polyps, and 590 subjects with no evidence of disease (NED). Opportunistic screening happens when potential subjects come to doctors for health examination or test due to illness or discomfort. The authors explained that “Doctors can use this opportunity to encourage these subjects to attend a disease screening program.”
The authors stated that “All subjects underwent a blood draw before colonoscopy and subsequent biopsies or surgery was performed. None of the subjects received chemotherapy, radiotherapy, or surgical intervention before the blood draw and colonoscopy.” Epi proColon® 2.0 CE assay was used to examine the blood level of SEPT9 gene methylation. The authors also explained that the “1/3 algorithm means that a sample was considered to be positive if at least one of the three PCRs were positive and was considered to be negative if all three PCR replicates were negative…[The] 2/3 algorithm means that a sample was considered to be positive if at least two of the three PCRs were positive and was considered to be negative if at least two of the three PCRs were negative.” Among the 388 CRC patients, 54.9% were at least age 60 years and 49.4% were women.
For the results, the positive detection rate (PDR) of the assay for stage 0 and I CRC were lower than later stages (Stage II, III and IV). The positive detection rate for CRC using the 1/3 algorithm was 82% and for adenoma, it was 36%. The authors reported that “The sensitivity was 57.7%, 63.5%, 87.7%, 86.6% and 89.5% for stage 0, I, II, III and IV, respectively, with 1/3 algorithm and 50.0, 53.8, 80.0, 77.4 and 84.2% for stage 0, I, II, III and IV, respectively, with 2/3 algorithm.” When evaluating for false positive rate for normal subjects by age group with the 1/3 algorithm (to yield more cases), no statistically significant change in PDR was observed, however, the authors reported that “the trend was quite clear before 59 years old. In contrast, a sharp increase in PDR to about 30% was observed at 60–69 age group and remained high until age over 80 years old. This observation indicates that the false PDR increased with the increase of age, and elder people exhibited higher false positive rate than younger people. To find out whether the trend is similar for CRC patients, we further examined the PDR for CRC subjects with identical age groups (2/3 algorithm…). The trend in CRC patients was similar to that of the normal subjects in age groups less than 59 years old, and….no sharp increase from 50 to 59 group to 60–69 group was found…”. No statistically significant difference in the PDR for CRC was found between males and females, and the PDR for CRC at various colorectal locations were essentially identical. They found that tests using 1/3 algorithm exhibited higher detection rate than those using the 2/3 algorithm for CRC, adenoma, hyperplastic polyps, while the false positive rate in subjects with NED was also higher with 1/3 algorithm. The authors did not acknowledge any limitations.
The authors concluded that algorithm, cancer stage and age are factors that can affect the detection rate of the SEPT9 assay, while sex and cancer location appeared to have no influence on its performance. The equal detection of CRC in both sexes and various colorectal locations facilitates the application of the assay in CRC screening.
Song L, Li Y, Jia J, et al. Algorithm Optimization in Methylation Detection with Multiple RT-qPCR. PLoS One. 2016 Nov 29;11(11):e0163333.
The aim of this opportunistic screening study was to show how algorithm choice impacts the use of the test and the indications for application. A total of 1133 subjects were recruited from three Chinese hospitals, including 369 CRC patients, 113 subjects with advanced adenoma, 87 subjects with polyps, 27 subjects with inflammatory bowel diseases (IBD), 47 subjects with other GI diseases (ulcer, colitis) and 490 subjects with no evidence of disease (NED). All 1133 subjects underwent a blood draw before colonoscopy and subsequent biopsies or surgery was performed. The authors reported that “None of the patients with cancer received chemotherapy, radiotherapy, or surgical intervention before the blood draw and colonoscopy.”
Blood samples from 1133 patients were tested using the triplicate Epi proColon® 2.0 assay for DNA extraction with various algorithms, which were compared to the newly developed single replicate SensiColon assay that measures methylation status of the same SEPT9 gene sequence. The new SensiColon assay, a single replicate SEPT9 assay, was recently approved by the Chinese FDA (CFDA) but it has not been approved by the US FDA. The authors explained that the “1/3 algorithm means that a sample was considered to be positive if at least one of the three PCRs were positive and was considered to be negative if all three PCR replicates were negative. The 2/3 algorithm means that a sample was considered to be positive if at least two of the three PCRs were positive and was considered to be negative if at least two PCRs were negative. The 3/3 algorithm means that a sample was considered to be positive if all three PCRs were positive and was considered to be negative if at least one PCR was negative.” Among the 369 CRC patients, 53.9% were at least 60 years old and 48% were women.
The results showed that the Epi proColon® 2.0 test, using the 1/3 algorithm, “showed the highest sensitivity (82.4%) for CRC cases at a lower specificity (82.0%) compared with the 2/3 algorithm (75.1% sensitivity, 97.1% specificity; p < 0.05) or 1/1 algorithm (71.3% sensitivity, 92.7% specificity; p < 0.001).” The specificity of the 3/3 algorithm was significantly higher that of the 1/3 (p < 0.001) and 1/1 (p < 0.001) algorithm. The sensitivity for each CRC stage using the 1/3 algorithm was 57.1% for Stage 0, 64.3% Stage I, 87.6% for Stage II, 87.8% for Stage III, and 93.3% for Stage IV. No significant difference in performance was found between the Epi proColon® 2.0 CE and the SensiColon assays for the detection of CRC. For instance, the sensitivity for CRC was 75.1% for the Epi proColon® test using the 2/3 algorithm compared to the sensitivity of 76.6% for the SensiColon using the 1/1 algorithm (p = 0.64). There was no difference between the two assays when compared across stages of CRC.
The authors acknowledged one limitation: “Since most cycle threshold (Ct) values from normal controls were not detected in the PCR reaction, the authors had to set the Ct values to 45 (the maximal number of PCR cycles that were run in the assay) for those undetected normal controls to plot the ROC (receiver operating characteristic) curve. This limitation led to the lack of specificity data points for Ct values >45. Therefore, no data were plotted above a certain percentage for 1-specificity (the X-axis) in the ROC (receiver operating characteristic) curves for both Epi proColon® 2.0 CE and SensiColon assays.”
The authors concluded that the choice of algorithm should depend on specific test usage, including screening and early detection. The optimal algorithm would be the one that best balances sensitivity and specificity. The application of an algorithm is dependent on the purpose of an assay. Screening for potential high-risk population normally needs high sensitivity while tests aiming at early detection normally require high specificity to avoid costly follow-up procedures. Their results can help to optimize the methylation detection in cancer screening and early detection.
Song L, Wang J, Wang H, et al. The quantitative profiling of blood mSEPT9 determines the detection performance on colorectal tumors. Epigenomics. 2018 Dec;10(12):1569-1583.
The aim of the comparative study was to investigate the quantitative relationship between the positive detection rate (PDR) in colorectal tumor detection and the mSEPT9 level to further understand the relationship between mSEPT9 level in blood and the severity of colorectal diseases. The type of study design was not mentioned. A total of 1347 subjects who were suspected of CRC and underwent subsequent colonoscopy examinations were recruited in this quantitative study from four hospitals located in China. Of the 1347 subjects, there were 465 CRC patients, 164 patients with adenoma (including 15 subjects with serrated adenoma [SA], 84 subjects with tubular adenoma [TA], 54 subjects with tubulovillous adenoma [TVA] and 11 subjects with villous adenoma [VA]), 108 patients with hyperplastic polyps (HP) and 610 normal subjects (no evidence of disease; NED). The authors reported that “The classification of all conditions was based on diagnosis from colonoscopy and subsequent pathological examinations… All subjects underwent a blood draw before colonoscopy and subsequent biopsies or surgery was performed. None of the subjects received chemotherapy, radiotherapy or surgical intervention before the blood draw and colonoscopy.” The level of blood mSEPT9 in various colorectal diseases was quantified by the Epi proColon® 2.0 assay. In the overall study, 35.8% were at least 60 years old and 44.5% were women.
For the results, PDR or sensitivity was positively correlated with the progression of colorectal tumors and the mSEPT9 level in an exponential relationship. For instance, when the positive detection rate was composed of CRC subjects at stage II (80.6%), III (77.4%) and IV (84.2%), the data showed that the PDR increased with the elevation of disease severity. No p value was shown. A strong correlation was found between mSEPT9 level and PDR or sensitivity in various tumor differentiation, pathological types or metastasis. For instance, the increase in PDR was coincident with the increase of mSEPT9 level, but no p value was shown. The receiver operating characteristic curves showed that the largest area under curve (AUC) of 0.81 was obtained when the CRC group is defined as positive and the NED group is defined as negative.
The authors acknowledged a study limitation in the use of mSEPT9 as screening biomarker: “The higher positivity of cancers at advanced stages leads to a detection bias towards advanced tumors that might not be curable, while a large proportion of earlier-stage localized tumors with high chance of cure are missed. This limitation is caused by the small amount of mSEPT9 in circulating tumor DNA (ctDNA) in early-stage cancer and the limit of detection of the methylation-specific PCR method.”
The authors concluded that the quantitative profiling of blood mSEPT9 determines the detection performance on colorectal tumors. Quantification of mSEPT9 may be applied to future risk assessment as an indicator for risk stratification and early detection, disease progression monitoring and evaluation of the therapeutic effect. The application of mSEPT9 could be extended from early screening to therapeutic effect monitoring and prediction in the near future.
Sun J, Fei F, Zhang M, et al. The role of mSEPT9 in screening, diagnosis, and recurrence monitoring of colorectal cancer. BMC Cancer. 2019 May 14;19(1):450.
The aim of the comparative study was to evaluate its utility in CRC screening and recurrence monitoring and to determine the diagnostic accuracy of mSEPT9 for colorectal cancer (CRC). The authors reported that “A total of 720 subjects including 600 cases of patients above 40 years old with high risk of CRC, 50 cases of preoperative patients who has been diagnosed with CRC and 70 cases of CRC patients after radical resection were recruited” by the Tianjin Union Medicine Center. “High-risk of CRC were defined as follows: at least one first-degree relative with CRC; having a history of intestinal adenoma or polyps; FOBT positive; having two or more of the following at the same time: chronic constipation, chronic diarrhea, mucus and bloody stool, history of adverse life events (such as divorce or death of relatives), history of chronic appendicitis or appendectomy, and history of chronic cholecystitis or cholecystectomy. These subjects were diagnosed by colonoscopy and subsequent pathological examinations.”
For screening and diagnosis of CRC, peripheral mSEPT9 detection and fecal occult blood test (FOBT) were performed in 650 subjects. The level of CEA, CA19–9 and CA724 was quantified in 173 subjects. The authors reported that “Blood samples of subjects with high risk of CRC were collected before colonoscopy examination. Blood samples of CRC patients who had taken colonoscopy examination were collected before surgery. An improved SEPT9 gene methylation assay (Epigenomics AG for Epi proColon® 2.0) was used for CRC detection….FOBT was performed one to 2 weeks before the detection of peripheral mSEPT9.” Among the 600 subjects with and without high risk of CRC, 59.5% were above 60 years of age and 52.5% were women.
For the results, the overall sensitivity for mSEPT9 CRC detection was 73.0% (95% confidence interval [CI] 60.1%-83.1%) at 94.5% (95% CI 92.0%-96.3%) specificity, and 17.1% of patients with intestinal polyps and adenoma were mSEPT9-positive at 94.5% specificity, which were higher than FOBT for the screening of CRC. The sensitivity for FOBT was 58.7% (95% CI 45.6–70.8%) and the specificity was 91.9% (95% CI 89.0%-94.1%). The authors also reported that “The sensitivity and specificity of mSEPT9 for diagnosis and recurrence monitoring were higher than that of CEA, CA19–9 and CA724. The combined detection of mSEPT9 and CECT enhanced the sensitivity for recurrence monitoring. Pre-therapeutic levels of mSEPT9 were strongly associated with TNM (tumor, nodes, metastases) stage, Dukes stages and mismatch repair deficiency (dMMR).”
The authors acknowledged several limitations, such as the numerous heterogeneities in the study, such as the different molecular markers for CRC, and small sample numbers of some of the clinicalpathological subgroups, such as the tumor staging subgroups.
The authors concluded that FOBT demonstrated low sensitivity for early screening of CRC. mSEPT9 analysis might be used as a routine biomarker for CRC screening. Thus, quantification of the peripheral mSEPT9 appears to be a simpler, cheaper, and more efficient tool for CRC screening. Their study indicated that peripheral mSEPT9 may be useful for the screening, early diagnosis, and recurrence monitoring of CRC.
Tóth K, Sipos F, Kalmár A, et al. Detection of methylated SEPT9 in plasma is a reliable screening method for both left- and right-sided colon cancers. PLoS One. 2012;7(9):e46000.
The aim of the retrospective comparative study was to describe the relationship of the sensitivity and specificity for the methylated Septin 9 (SEPT9) test to colorectal cancer (CRC) cancer localization, guaiac-based fecal occult blood test (gFOBT) and carcinoembryonic antigen (CEA). The overall comparative study design was not further specified. The study was located in Europe in Hungary and Germany. The study sites were not defined. The study excluded patients with: systemic inflammatory, malabsorptive diseases, acute medical conditions, and other malignant diseases. The authors reported that “All of the subjects (healthy controls and patients with colorectal cancer) underwent lower endoscopy, during which biopsies were taken for histological examination…None of the patients with cancer received chemotherapy, radiotherapy, or surgical intervention before endoscopy.”
Plasma samples were collected for SEPT9 analysis from patients with no evidence of disease (NED) (n = 94) before colonoscopy and CRC (n = 93) before surgical treatment; however, two NED subjects resulted in a positive result and one CRC patient had a negative result and were excluded from the study. The authors reported that “DNA was isolated using Epi proColon kit 2.0. Qualitative determination was performed using Epi proColon® 2.0 RT-PCR assay…The advantages of Epi proColon® 2.0 kit are fewer handling steps, shorter time to result and increased clinical performance compared to the first generation test Epi proColon® 1.0….Samples for gFOBT and CEA analysis were collected retrospectively from NED (n = 17 and 27, respectively) and CRC patients (n = 22 and 27, respectively).” Among the 93 cancer patients, the mean age was 67.8 ± 9.8 years and 48.4% were women.
For the results, the specificity and sensitivity of Septin 9 for CRC was 84.8% (95% confidence intervals [CI] 75.8% to 91.4%) and 95.6% (95% CI 89.2% to 98.8%), respectively. Thus, “the SEPT9 test was positive in 15.2% (14/92) of NED and 95.6% (88/92) of CRC, including 100% (67/67) from stage II to stage IV CRC and 84% (21/25) of stage I CRC when a sample was called positive if 1 out of 3 PCR replicates was positive. In a second analysis (2 positive results out of 3 PCR replicates) specificity improved to 99% (91/92, 95% CI 94.1–100) of NEDs, at a sensitivity of 79.3%” (73/92, 95% CI 69.6–87.1) of SEPT9 positives in CRC.
gFOBT was positive in 29.4% (5/17) of healthy NED subjects and 68.2% (15/22) of CRC patients and elevated CEA levels were detected in 14.8% (4/27) of healthy NED subjects and 51.8% (14/27) of CRC subjects. Thus, the specificity and sensitivity of gFOBT for CRC was 70.6% (95% CI 44% to 89.7%) and 68.2% (95% CI 45.1% to 86.1%), respectively. The specificity and sensitivity of CEA for CRC was 85.2% (95% CI 66.3% to 95.8%) and 51.8% (95% CI 31.9% to 71.3%), respectively. Both SEPT9 (84.8%) and CEA (85.2%) showed higher specificity than gFOBT (70.6%).
CRC samples were then divided into left- and right-sided cancers, and in the course of this comparison no significant (p = 0.65) difference was found between the two groups. SEPT9 was positive in 96.4% (54/56) of left-sided colon cancer (LSCC) cases and 94.4% (34/36) of right-sided colon cancer (RSCC) cases. gFOBT was positive in 83.3% (10/12) of cases with LSCC and 50% (5/10) of cases with RSCC, elevated CEA was detected 60% (9/15) of LSCC and 41.7% (5/12) of RSCC. The authors did not acknowledge any limitations.
The authors concluded that” the high degree of sensitivity and specificity of SEPT9 in plasma makes it a better method to detect CRC than gFOBT and CEA, even for the more difficult to detect RSCC…This marker was more sensitive and specific than gFOBT and CEA and did not show any differences between left- and right-sided colon cancers. Hence, the Septin 9 marker may be a safe and useful test for CRC screening.”
Warren JD, Xiong W, Bunker AM, et al. Septin 9 methylated DNA is a sensitive and specific blood test for colorectal cancer. BMC Med. 2011 Dec 14;9:133.
The aim of the study was to demonstrate the performance of an improved sensitivity blood-based Septin 9 (SEPT9) methylated DNA test for colorectal cancer. In a case-control study, plasma samples were collected from 50 untreated CRC patients at one U.S. and two Russian institutions, and 94 control samples from CRC-free patients were collected at four U.S. institutions within one year of having a negative colonoscopy. The authors reported that “In a small prospective cohort study, blood specimens were collected from 306 asymptomatic patients undergoing routine screening colonoscopy at a single community clinic in the U.S…. SEPT9 methylated DNA concentration was tested in analytical specimens, plasma of known CRC cases, healthy control subjects, and plasma collected from colonoscopy patients…For the comparison study, the PCR method was performed as described in the Epi proColon® test.” For the case control study, the average age of the cancer patients was 62 (range: 42 to 85) years. Control subjects had an average age of 58 (range: 40 to 86) years. For the prospective study, the average age of the asymptomatic cohort was 56 (range: 22 to 84) years, with 195 (63.7%) of these were 50 to 75 (average 59) years of age.
For the results from the case-control study, the authors reported that the “test had an overall sensitivity for CRC of 90.0% (95% confidence interval [CI], 77.4% to 96.3%) and specificity of 88.3% (95% CI, 79.6% to 93.7%) detecting CRC in patients of all stages. For early stage cancer (I and II) the test was 86.8% (95% CI, 71.1% to 95.1%) sensitive. The test identified CRC from all regions, including proximal colon (for example, the cecum) and had a 12% false-positive rate. In the small prospective cohort study, the SEPT9 test detected 12% of adenomas with a false-positive rate of 3%.” The authors did not acknowledge any study limitations.
The authors concluded that the improved SEPT9 methylated DNA test was more sensitive than previously described methods. A sensitive blood-based CRC screening test using the SEPT9 biomarker specifically detects a majority of CRCs of all stages and colorectal locations. The test could be offered to individuals of average risk for CRC who are unwilling or unable to undergo colonoscopy.
Yang X, Xu ZJ, Chen X, et al. Clinical value of preoperative methylated septin 9 in Chinese colorectal cancer patients. World J Gastroenterol. 2019 May 7;25(17):2099-2109.
The aim of the study was to describe the diagnostic and prognostic role of preoperative serum mSEPT9 for colorectal cancer (CRC) in Chinese patients. A retrospective analysis of 354 study patients, of which 300 had histologically confirmed CRC and 54 were normal, was performed in China. This study was conducted among patients at the Department of Hepatobiliary and Enteric Surgery in Xiangya Hospital. A total of 354 subjects with mSEPT9 serum detection before surgery were recruited from a medicine-pharmacy-nursing integrative parenteral medication rational use and safety early warning platform, the Parenteral Prescription Early Warning and Assessment System. Patients’ characteristics, treatments, and laboratory data, including age, the date of surgery, Union for International Cancer Control (UICC) stages, and distant metastasis (M) were collected. The authors reported that “Progression-free survival (PFS) time was calculated for the study population from the CRC patients’ date of surgery to presentation of clinical or pathological evidence of cancer recurrence.”
Methylation levels of SEPT9 were quantified by quantitative, methylation-specific polymerase chain reaction before surgery. A 10 mL peripheral blood sample was collected for the SEPT9 assay. The mSEPT9 was assayed with the Epi proColon® 2.0 kit.
Additionally, the effects of mSEPT9 on the occurrence and prognosis of 330 CRC cases from The Cancer Genome Atlas (TCGA) database were evaluated using bioinformatics analyses. The authors reported that “The CRC cases were selected and analyzed retrospectively. Patients whose mSEPT9 levels were less than or equal to median were assigned to the low mSEPT9 group, whereas others were assigned to the high mSEPT9 group. The overall survival (OS) time for the TCGA database was calculated from the CRC patients’ date of surgery to the date of dead or to the last contact date.” Among the 300 Chinese CRC study, 65% were above age 50 years and 46.5% were women.
The results showed that the Chinese patients with positive mSEPT9 showed a tendency toward lower PFS. For the prognostic significance of mSEPT9 in Chinese CRC patients, Kaplan-Meier univariate analysis showed that positive mSEPT9 was associated with shorter PFS among the Chinese CRC patients compared to negative mSEPT9 CRC patients (P = 0.019). The positive mSEPT9 CRC cases were estimated to have a mean PFS duration of 3.7 months (95% confidence interval [CI]: 2.14-5.19) compared with the 6.0 months (95% CI: 0-13.87) in the negative mSEPT9 CRC cases.
Other results showed that “the preoperative serum mSEPT9 levels were statistically significantly higher in Chinese CRC patients than in the normal subjects (P = 0.008). The positive rate of mSEPT9 was 52.3% for the Chinese CRC patients and 25.9% for normal subjects (P = 0.102).” mSEPT9 levels showed a significant increase from UICC stages II to III (P = 0.033) and stages III to IV (P < 0.0001), but no statistically significant difference was detected between stages I to II (P = 0.898). A positive mSEPT9 test in the Chinese study was strongly associated with advanced UICC stages, deeper invasion by the primary tumor, and more distant metastasis.
“Methylation levels of SEPT9 were stage-dependent and showed a stepwise increase in UICC stages (I–IV), primary tumor categories (T1–T4), regional node categories (N0–N2), and distant metastasis categories (M0–M1).”
Among 351 patients from the TCGA database, the serum mSEPT9 levels of 330 CRC patients were higher than those of the 21 normal subjects, but were not statistically significant (P = 0.530). Serum mSEPT9 showed prognostic significance for the CRC patients from the TCGA database (P = 0.008) with patients that had high mSEPT9 levels showing a tendency toward lower OS. CRC patients with low mSEPT9 levels were found to be correlated with longer OS. The low mSEPT9 CRC cases had an estimated mean OS duration of 8.1 months (95% CI: 6.53-9.27) compared with the 5.1 months (95% CI: 3.87-6.33) in the high mSEPT9 CRC cases. After analyzing TCGA clinical data, the high mSEPT9 group was found to be correlated only with more distant metastasis.
The authors acknowledged the limitations that their study compared two different study populations. The study population was Chinese, while patients from the TCGA database were who were from White, American Indian, Asian, or African American populations.
The authors concluded that mSEPT9 was proven to be an effective biomarker for diagnosis, recurrence, and prognosis of CRC in Chinese patients. mSEPT9 analysis may add valuable information to current tumor staging. Serum mSEPT9 in Chinese CRC patients appears to be a powerful diagnostic tool and offers promising novel prognostic markers. Patients with initially high mSEPT9 levels may benefit from intensive therapy and close monitoring of disease development and recurrence.
4. Medicare Evidence Development & Coverage Advisory Committee (MEDCAC)
A MEDCAC meeting was not convened on this issue.
5. Evidence-Based Guidelines
US Preventive Services Task Force. Draft Recommendation Statement: Colorectal Cancer: Screening. October 27, 2020. Accessed link December 22, 2020: https://uspreventiveservicestaskforce.org/uspstf/draft-recommendation/colorectal-cancer-screening3.
Note: This is a draft recommendation. At the time of this assessment, it has not been finalized.
On October 27, 2020, the USPSTF published a draft recommendation statement on colorectal cancer screening that was open for public comment until November 23, 2020. The USPSTF recommends screening for colorectal cancer in all adults ages 50 to 75 (grade A recommendation). The USPSTF recommends screening for colorectal cancer in adults ages 45 to 49 years (grade B recommendation). As part of the systematic review, the USPSTF concluded with high certainty that the net benefit of screening for colorectal cancer in adults ages 50 to 75 years was substantial. The USPSTF concluded with moderate certainty that the net benefit of screening for colorectal cancer in adults ages 45 to 49 years was moderate.
In the systematic review requested by the USPSTF, the authors found that “Serum testing for circulating mSEPT9 in one study appears to have slightly lower sensitivity and lower specificity to detect CRC than commonly evaluated/employed FITs” and concluded that future research is needed. “In particular, [for] promising serum tests are (sic) [such as] Epi proColon which has a single adequately powered test accuracy study with sensitivity at or below, and specificity much below commonly studied FITs” (Lin, 2020).
The 2020 draft recommendation reported that “more research is needed on the accuracy and effectiveness of emerging screening technologies such as serum- and urine-based colorectal cancer screening tests and capsule endoscopy tests to potentially improve acceptance and adherence to colorectal cancer screening, if found to be accurate and effective” (USPSTF Draft Recommendation, 2020). The Task Force concluded that “This assessment of net benefit applies to stool-based tests with high sensitivity, colonoscopy, computed tomography (CT) colonography, and flexible sigmoidoscopy. See Table 1 for characteristics of recommended screening strategies. The USPSTF recommendation for screening for colorectal cancer does not include serum tests [i.e., blood-based tests], urine tests, or capsule endoscopy for colorectal cancer screening because of the limited available evidence on these tests, and because other effective tests (i.e., the recommended screening strategies) are available” (USPSTF Draft Recommendation, 2020).
US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2016 Jun 21;315(23):2564-2575.
The USPSTF reviewed “the evidence on the effectiveness of screening with colonoscopy, flexible sigmoidoscopy, computed tomography colonography, the guaiac-based fecal occult blood test, the fecal immunochemical test, the multitargeted stool DNA test, and the methylated SEPT9 DNA test in reducing the incidence of and mortality from colorectal cancer or all-cause mortality; the harms of these screening tests; and the test performance characteristics of these tests for detecting adenomatous polyps, advanced adenomas based on size, or both, as well as colorectal cancer.”
The USPSTF found convincing evidence that screening for colorectal cancer in adults aged 50 to 75 years reduces colorectal cancer mortality; screening average-risk, asymptomatic adults in this age group yields a substantial net benefit. The USPSTF found several different methods can accurately detect early stage colorectal cancer and adenomatous polyps and reported that “Multiple screening strategies are available to choose from, with different levels of evidence to support their effectiveness, as well as unique advantages and limitations, although there are no empirical data to demonstrate that any of the reviewed strategies provide a greater net benefit.”
Because at the time of their review, the USPSTF found no head-to-head studies, they reported a lack of evidence demonstrating that any of the screening strategies were considered more effective than others. The different screening strategies are listed in the table on the Characteristics of Colorectal Cancer Screening Strategies (not presented in any preferred or ranked order). The methylated SEPT9 DNA test is not listed in this table (USPSTF, 2016).
The USPSTF (2016) recommends the following:
- Screening for colorectal cancer starting at age 50 years and continuing until age 75 years (A recommendation).
- The decision to screen for colorectal cancer in adults aged 76 to 85 years should be an individual one, taking into account the patient’s overall health and prior screening history (C recommendation).
methylated SEPT9 DNA test
When describing the characteristics of the colorectal cancer screening strategies, a footnote states that “[a]lthough a serology test to detect methylated SEPT9 DNA was included in the systematic evidence review [Lin, 2016], this screening method currently has limited evidence evaluating its use (a single published test characteristic study met inclusion criteria, which found it had a sensitivity to detect colorectal cancer of <50%). It is therefore not included in this table [on Characteristics of Colorectal Cancer Screening Strategies]” (USPSTF, 2016).
Regarding serology tests, the task force stated “The FDA approved a blood test to detect circulating methylated SEPT9 DNA (Epi proColon®; Epigenomics) in April 2016. [PMA for Epi proColon®. Accessed April 21, 2016] A single test characteristic study met the inclusion criteria for the systematic evidence review supporting this recommendation statement; it found the SEPT9 DNA test to have low sensitivity (48%) for detecting colorectal cancer. [Church, 2014]” (USPSTF, 2016).
Lin JS, Piper MA, Perdue LA, et al. Screening for Colorectal Cancer: A Systematic Review for the U.S. Preventive Services Task Force [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Jun.
Lin and colleagues (2016) reported the results of a systematic review to inform the USPSTF 2016 recommendations. The authors summarized the evidence for methylated SEPT9 DNA testing: “[t]hus far, only one blood test, which detects circulating methylated SEPT9 DNA, has been prospectively evaluated in a screening population. This test had a sensitivity of only 48.2 percent (95% CI, 32.4 to 63.6) to detect CRC”.
In the systematic review of blood tests, the authors identified only one diagnostic accuracy study (Church, 2014) that met their inclusion criteria that evaluated mSEPT9. The authors found that “[o]nly one blood test has been prospectively evaluated in a screening population.[Church, 2014] This test detects circulating methylated SEPT9 DNA. This test was evaluated through a fair-quality, multicenter diagnostic accuracy study (n=1,516) that found that mSEPT9 had a relatively low sensitivity to detect CRC (48.2% [95% CI, 32.4 to 63.6]), with a test positivity of 10.1 percent.”
Specifically, they “found only one study that evaluated the test performance of a blood test to screen for CRC in asymptomatic, average-risk adults. This fair-quality multicenter prospective nested case-control study (Prospective Evaluation of Septin 9 or PRESEPT), evaluated the mSEPT9 marker using the first generation of a commercially available polymerase chain reaction assay, Epi proColon® (Epigenomics, Germantown, MD).[Church, 2014] The assay was designed to detect circulating methylated SEPT9 DNA as a marker for CRC (not precursors of CRC).”
For the methods, “[t]his study initially included 7,920 asymptomatic adults from 32 clinical sites in the United States and Germany who met inclusion criteria, were age 50 years or older, and had an average risk for CRC. This study excluded persons with previous colonoscopy, previous cancer or adenomas, iron deficiency anemia, blood in stool, or family history of CRC. Eighty-seven percent of persons were available for analyses, with attrition mainly due to incomplete data or inadequate sample quality. Of the participants available for analyses (n=6,874), the mean age was 61 years, 55 percent were women, and the prevalence of underlying CRC was 0.8 percent. Participants had their blood drawn for the mSEPT9 assay at least 1 day before the colonoscopy bowel preparation, with an average of 14 days prior to preparation. All patients included in the analyses had colonoscopies performed by board-certified endoscopists at the respective clinical site. The overall adenoma detection rate was 44.8 percent. It is assumed but not reported that the endoscopist was blinded to mSEPT9 assay test results. Interpretation of the mSEPT9 assay was independent of colonoscopy and pathology findings.”
For results from “the analyses, study investigators identified a subset of persons (n=1,516) using random sampling stratified by colonoscopy findings, including all 53 cancers, 315 of the 666 advanced adenomas, 210 of the 2,359 nonadvanced adenomas, and 938 of the 3,796 persons without evidence of disease. The test positivity rate in this subset was 10.1 percent (153/1,510). Weighted sensitivity and specificity of the mSEPT9 assay to detect CRC calculated from this subset was 48.2 percent (95% CI, 32.4 to 63.6) and 91.5 percent (95% CI, 89.7 to 93.1), respectively. Test sensitivity to detect CRC increased with increasing CRC tumor stage. Sensitivity for distal (53.3% [95% CI, 34.7 to 72.4]) and proximal CRC (39.4% [95% CI, 14.2 to 68.2]) was not statistically significantly different (p=0.28). Test sensitivity to detect advanced adenomas was 11.2 percent (95% CI, 7.2 to 15.7); however, the assay was not designed to detect advanced adenomas.”
The authors concluded that “[a]lthough a blood test would undoubtedly increase screening rates, the Epi proColon® test for circulating mSEPT9 has worse test performance for the detection of CRC than other noninvasive testing” and that for future research needs, “additional diagnostic accuracy studies of screening tests incorporating new technologies with a limited evidence base (e.g., mtsDNA, serum mSEPT9) is also needed, with reporting of percent inadequate or indeterminant results.”
Wolf AMD, Fontham ETH, Church TR, et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 2018 Jul;68(4):250-281.
For this guideline update, the American Cancer Society (ACS) used an existing systematic evidence review of the CRC screening literature by the US Preventive Services Task Force (USPSTF) for its 2016 CRC screening recommendation update as sources and microsimulation modeling analyses from the Cancer Intervention and Surveillance Modeling Network (CISNET) CRC group. In addition, literature searches were conducted to identify relevant new studies that have addressed screening outcomes since completion of the USPSTF evidence review. The ACS Guideline Development Group applied the Grades of Recommendations, Assessment, Development, and Evaluation (GRADE) and GRADE Evidence-to-Decision (EtD) criteria in formulating and assigning the strength of recommendations.
The American Cancer Society Guideline for CRC Screening (2018) Recommendations are:
- The ACS recommends that adults aged 45 y and older with an average risk of CRC undergo regular screening with either a high-sensitivity stool-based test or a structural (visual) examination, depending on patient preference and test availability. As a part of the screening process, all positive results on noncolonoscopy screening tests should be followed up with timely colonoscopy.
- The recommendation to begin screening at age 45 y is a qualified recommendation.
- The recommendation for regular screening in adults aged 50 y and older is a strong recommendation.
- The ACS recommends that average-risk adults in good health with a life expectancy of greater than 10 y continue CRC screening through the age of 75 y (qualified recommendation).
- The ACS recommends that clinicians individualize CRC screening decisions for individuals aged 76 through 85 y based on patient preferences, life expectancy, health status, and prior screening history (qualified recommendation).
- The ACS recommends that clinicians discourage individuals over age 85 y from continuing CRC screening (qualified recommendation).
Options for CRC screening
Stool-based tests
- Fecal immunochemical test every y
- High-sensitivity, guaiac-based fecal occult blood test every y
- Multitarget stool DNA test every 3 y
Structural examinations
- Colonoscopy every 10 y
- CT colonography every 5 y
- Flexible sigmoidoscopy every 5 y
The ACS recommendation is a general overall recommendation for CRC screening and does not recommend use of a specific individual test.
mSept9 DNA
In the ACS review of mSept9 tandem studies (Church, 2014; Johnson, 2014; Potter, 2014) comparing advanced neoplasia detection rates with a conventional CRC screening test, they found that “[a]lthough these studies demonstrate improving test sensitivity, concerns remain about poor specificity compared with recommended screening options and the limited base of evidence in asymptomatic, screening populations…In addition, mSept9 is a novel blood test for CRC early detection with no comparable screening tests from which to infer a benefit in terms of critical outcomes (CRC mortality or incidence reduction), as there are for the included screening test options. Importantly, the test has not been cleared by the FDA for unrestricted use in general routine screening.” (Wolf, 2018). The ACS concludes that “based on the limitations noted above [in the ACS guideline document], at this time, mSept9 is not included in this guideline as an option for routine CRC screening for average-risk adults.” (Wolf, 2018). The methylated Sept9 DNA test is not among the list of recommended CRC screening options but has been cleared by the FDA for use in special circumstances.
6. Professional Society Recommendations / Consensus Statements / Other Expert Opinion
Rex DK, Boland CR, Dominitz JA, et al. Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2017 Jul;112(7):1016-1030.
The authors “suggest that the Septin9 serum assay (Epigenomics, Seattle, Wash) not be used for screening (weak recommendation, low-quality evidence).”
For the Septin9 assay, the authors reported that “[t]he first FDA-approved serum test for CRC screening is the Septin9 assay (Epigenomics, Seattle, Wash). In a large screening colonoscopy study, this test had a sensitivity of 48% for detection of CRC and no sensitivity for detection of precancerous polyps [Church, 2014]. The test is expensive relative to FIT. The advantage of the Septin9 test is that it is a serum assay and is at least potentially more convenient for patients. Some patients who refused colonoscopy preferred this test over FIT (103). Disadvantages of the Septin9 assay are markedly inferior performance characteristics compared with FIT, including lower sensitivity for cancer, inability to detect advanced adenomas (104), and low cost-effectiveness relative to other screening tests (105). The test appears to have higher sensitivity for late-stage compared with early-stage cancer [Church, 2014]. The willingness of patients with positive Septin9 tests to undergo colonoscopy remains uncertain. The uncertainties regarding the true clinical utility of Septin 9 makes shared decision-making difficult. Clinicians should inform patients of the uncertain benefits of this test on CRC mortality, the inability of the assay to detect polyps, and the array of superior alternatives. The best frequency for performing the test is uncertain. Given these limitations, the MSTF (the U.S. Multi-Society Task Force of Colorectal Cancer) suggests that Septin9 not be used for screening.” They also state that “[a]s an extreme example [of not offering the ‘best’ test], the MSTF considers that equating the Septin9 assay with colonoscopy would be a disservice to patients, because the sensitivity of colonoscopy for cancer and advanced lesions exceeds that of Septin9 by a very large margin.”
NCCN (National Comprehensive Cancer Network). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Colorectal Cancer Screening. Version 2.2019. August 2, 2019. Accessed February 5, 2020.
In a summary algorithm table for Risk Assessment for Colorectal Cancer under Screening Modality and Schedule, a footnote states that a “blood test that detects circulating methylated SEPT9 DNA has been FDA-approved for CRC screening for those who refuse other screening modalities. It is not recommended for routine screening. The interval for repeating testing is unknown.”
An emerging option for CRC screening is a blood-based screening test. The authors report that “the methylation status of the septin9 (SEPT9) gene has been shown to distinguish CRC tissue from normal surrounding tissue, and circulating methylated SEPT9 DNA in plasma is a biomarker for CRC.132-135 A multicenter center compared the FIT test and a SEPT9 DNA methylated blood test for CRC screening of 102 patients with identified CRC, and found that the specificity for CRC detection was higher for FIT (97.4% vs. 81.5%, respectively) but the sensitivity for CRC detection was not significantly different (68% vs. 73.3%, respectively) [Johnson, 2014]. Another clinical trial comparing the uptake of the methylated SEPT9 DNA blood-based test to FIT for CRC screening in 413 average-risk adults found that more participants took the blood test (99.5% vs. 88.1%; p < .001).137 In 2016, a blood test that detects circulating methylated SEPT9 DNA was approved by the FDA and may provide an alternative for individuals who refuse other screening modalities. The sensitivity of the SEPT9 DNA test for the detection of CRC has been reported to be 68% with a specificity of 80% [Potter, 2014]. Factors that may potentially negatively impact the performance of the SEPT9 DNA test have been suggested, including early-stage disease, age > 65 years, diabetes, arteriosclerosis, and arthritis [Ørntoft, 2015]. The interval for repeat testing is uncertain and the NCCN Guidelines for CRC Screening (see CSCR- 2 and CSCR-3 in the algorithm) do not recommend the SEPT9 DNA test for routine screening.”
The references that are full citations with author and year are studies that administered the Epi proColon® test.
NCCN (National Comprehensive Cancer Network). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Colorectal Cancer Screening. Version 1.2020. April 22, 2020. Accessed April 30, 2020.
In the algorithm diagram about Screening Modality and Schedule on page CSCR-3 and CSCR-4, the footnote indicates that “[a] blood test that detects circulating methylated SEPT9 DNA has been FDA-approved for CRC screening for those who refuse other screening modalities. It is not recommended for routine screening. The interval for repeating testing is unknown.” The same footnote appears in the Screening Modality and Schedule section (page CSCR-A, 2 of 5) under the table that shows the sensitivity and specificity of individual screening tests. However, the blood-based mSEPT9 DNA test is not listed in the table reporting sensitivity and specificity; thus, the sensitivity and specificity of the mSEPT test is not shown.
The NCCN guideline in the Screening Modality and Schedule section (page CSCR-A, 5 of 5) is under a heading:
mSEPT9 blood test
- Not recommended for routine screening. Can be considered for patients who refuse other screening modalities.
It should be noted that the mSEPT9 DNA test is not listed in the algorithm diagram as a screening modality under stool-based tests along with high-sensitivity guaiac-based or immunochemical-based testing or FIT-DNA-based testing, but it is listed as a footnote underneath the screening modality and schedule flow diagram.
In the Discussion under the heading “Emerging Options: Blood-Based Screening Test”, the authors report that “[t]he methylation status of the septin9 (SEPT9) gene has been shown to distinguish CRC tissue from normal surrounding tissue, and circulating methylated SEPT9 DNA in plasma is a biomarker for CRC.132-135 A multicenter study compared the FIT test and a SEPT9 DNA methylated blood test for CRC screening of 102 patients with identified CRC, and found that the specificity for CRC detection was higher for FIT (97.4% vs. 81.5%, respectively) but the sensitivity for CRC detection was not significantly different (68% vs 73.3%, respectively).136 Another clinical trial comparing the uptake of the methylated SEPT9 DNA blood-based test to FIT for CRC screening in 413 average-risk adults found that more participants took the blood test (99.5% vs 88.1%; p < 0.001).137”
The authors further explain that “[i]n 2016, a blood test that detects circulating methylated SEPT9 DNA was approved by the FDA and may provide an alternative for individuals who refuse other screening modalities. The sensitivity of the SEPT9 DNA test for the detection of CRC has been reported to be 68% with a specificity of 80%.138 Factors that may potentially negatively impact the performance of the SEPT9 DNA test have been suggested, including early-stage disease, age > 65 years, diabetes, arteriosclerosis, and arthritis.139 The interval for repeat testing is uncertain and the NCCN Guidelines for CRC Screening (see CSCR-[3] and CSCR-[4] in the algorithm) do not [recommend] the SEPT9 DNA test for routine screening.” (NCCN, 2020)
7. Public Comment
Public comments sometimes cite the published clinical evidence and give CMS useful information. Public comments that give information on unpublished evidence such as the results of individual practitioners or patients are less rigorous and therefore less useful for making a coverage determination.
CMS uses the initial public comments to inform its proposed decision. CMS responds in detail to the public comments on a proposed decision when issuing the final decision memorandum. All comments that were submitted without personal health information may be viewed in their entirety by using the following link https://www.cms.gov/medicare-coverage-database/details/nca-view-public-comments.aspx?NCAId=296.
Initial Comment Period: 2/28/2020-3/29/2020
During the initial 30-day public comment period, CMS received 67 comments; two of which were secondary comments in response to other comment letters. The vast majority of comments supported coverage of blood-based biomarker screening tests for colorectal cancer screening (CRC) and/or Epi proColon® specifically. Commenters noted that blood-based biomarker screening tests are easier tests and promote higher compliance in the unscreened or non-compliant population. While one commenter supported coverage of blood-based biomarker screening tests they support waiting for the USPSTF’ final review before finalizing the NCD. Many of the comments were supportive of developing coverage criteria for blood-based CRC screening tests rather than coverage of a specific test. Several manufacturers commented that they have a blood-based biomarker test for CRC screening in development. However, since Epi proColon® is the first FDA-approved blood-based biomarker test many of the comments were specific to this test. Several commenters did not support coverage of Epi proColon® citing concerns around its clinical performance including lack of sensitivity and specificity, annual screening interval and consequent increase in colonoscopy referrals.
The majority of comments were provided by physicians, other health care professionals, laboratories, patient advocacy organizations and biotechnology manufacturers.
Second Comment Period: 10/16/2020-11/15/2020
During the 30-day comment period following the release of the proposed NCD and decision memorandum, CMS received 173 comments; 15 of which were omitted from publication on the CMS website due to personal health information content. Of these comments, 113 were statements of support for the Epi proColon® test without providing specifics. All but two commenters were supportive of the approach to expand colorectal cancer screening to include blood-based biomarker tests rather than test by test consideration. These commenters favored retaining the traditional pathway for coverage. While commenters were supportive of the expansion of CRC screening, they expressed concerns regarding the proposed test criteria, with many suggesting modifications. Specifically, the commenters disagreed with setting a specific test performance threshold and requiring inclusion in a professional society guideline or consensus statement or USPSTF recommendation. Many commenters questioned why modeling data was not included in the analysis section. Commenters were not supportive of the Epi proColon® test not meeting the proposed test criteria. Commenters also challenged the test interval, particularly the FDA label indicating a specific test interval and many suggested alternatives. Some commenters suggested lowering the minimum patient age limit to correspond with recently published guidelines. Detailed summaries of all submitted comments with CMS responses are included below.
Sixteen comments were provided by healthcare professionals and physicians, one of which included a comment submitted on behalf of the Early Detection Research Network (EDRN), which represented twelve physicians. Thirteen comments were from biotechnology manufacturers including three from Polymedco Cancer Diagnostics, two from Epigenomics; one of which was in response to another public comment, Exact Sciences, Clinical Genomics, Guardant Health, CellMax, GRAIL, Freenome, Roche Diagnostics and an unidentified IVD company. Five comments were from non-profit/advocacy organizations including Colon Cancer Foundation, Fight Colorectal Cancer (CRC), Colon Cancer Coalition, Personalized Medicine Coalition (PMC), and The Coalition for 21st Medicine (C21). Four comments were provided by professional associations including AdvaMed, Association of Molecular Pathologists (AMP), American Cancer Society (ACS) and ACS Cancer Action Network, and College of American Pathologists (CAP). The remaining seven comments were provided by two clinical laboratories, two medical centers, a consultant, an independent researcher and a financial analyst.
Numerous articles were submitted with public comments that were not available or considered for the proposed decision. These articles have been reviewed and those that fall within the scope of this NCD as well as our literature search and review parameters have been considered in the analysis section.
Expansion of Colorectal Cancer Screening
Comment: Commenters expressed their support for expanding colorectal cancer screening and stressed the importance of prevention and screening. The vast majority of commenters were supportive of the coverage approach to provide a path forward by reducing the administrative burden for both CMS and test manufacturers while increasing access to testing.
Response: We agree with the importance of prevention and screening. We appreciate the supportive comments for expanding colorectal cancer screening for Medicare beneficiaries.
Comment: Two commenters favored CMS assessing new screening tests by retaining the traditional pathway for test by test consideration and noted that other factors such as setting, screening uptake and adherence to follow-up may be important to consider on an individual basis.
Response: While we have focused on sensitivity and specificity, we recognize the importance of these other factors in evaluating a screening test and consider these factors in our determinations as noted in the background section. We are aware that there are several promising screening tests in development or evaluation stages and believe that Medicare beneficiaries should have timely appropriate access to innovative tests. The pathway that we have established will also provide clarity to innovators and assurance that the screening test has high sensitivity and specificity. Based upon new evidence, stakeholders may submit a reconsideration request accordingly. The information to request an NCD can be viewed at: https://www.cms.gov/Medicare/Coverage/DeterminationProcess/howtorequestanNCD.
Comment: One commenter encouraged CMS to consider a coverage framework that would enable circulating tumor DNA (ctDNA) screening in other populations such as lung and breast cancer.
Response: We appreciate the comment but this issue is outside the scope of this NCD, which is limited to colorectal cancer screening tests. The information to request an NCD can be viewed at: https://www.cms.gov/Medicare/Coverage/DeterminationProcess/howtorequestanNCD.
Comment: One commenter stated that this NCD should cover both liquid biopsy and stool-based assays on a rolling basis to prevent NCDs for advanced stool-based assays from becoming outdated. Another commenter suggested an NCD for non-invasive surveillance testing.
Response: We are not adopting these comments at this time as the issues raised are outside the scope of this national coverage analysis. The scope of this NCD is for CRC screening using blood-based biomarker tests. The information to request an NCD can be viewed at: https://www.cms.gov/Medicare/Coverage/DeterminationProcess/howtorequestanNCD.
Pandemic Impact:
Comment: A few commenters also commented on the impact the pandemic has had on screening.
Response: We understand the effect the pandemic has had on patient access and remind patients of the non-invasive CRC screening Medicare covers such as screening fecal occult blood test (FOBT), fecal immunochemical test (FIT) and Cologuard™.
Non-Compliance/Adherence
Comment: Many commenters expressed that despite all the outreach, compliance for CRC screening is low. They cited many reasons for patients either not wanting or not willing to get a colonoscopy. Some commenters stated that patients find stool-based testing unpleasant.
Response: We appreciate the insightful comments. Since the 1990s, Medicare has covered a number of CRC screening tests from non-invasive fecal based tests to colonoscopy, providing a range of choices for patients to choose the most individually suitable modalities. We agree that patient adherence is important to successful CRC prevention and improvements in health outcomes. Medicare covers a menu of screening options including a stool DNA test that offers a simplified approach to sample collection.
Comment: Many commenters pointed out that CMS did not include adherence as a test performance characteristic. They stated that the best test is the one that gets done and that an imperfect test is better than no test. Many commenters stated that patients view blood tests as easier and would be more willing to get screened with a blood test.
Response: We understand the concerns regarding adherence. There are a number of factors to consider in addition to adherence. Increased adherence because of more convenience to a lower performance CRC screening test may lead to missing more cases of colorectal cancer and more unnecessary diagnostic colonoscopies when compared to the currently recommended (by societies and USPSTF) and FDA approved non-invasive screening tests, such as FIT and the stool DNA test, for routine screening of colorectal cancer. The overall goal is to prevent CRC or identify those cancers early to and reduce morbidity and mortality of colorectal cancer by considering and balancing all relevant factors.
In the Analysis section above on Harms of Lower Performance Screening for CRC Testing that was about screening test false positive and false negative rates, the discussion had a focus on screening test error rates. The purpose of this discussion was to describe the harms of the false positive and the false negative test result from a one-time screening using Epi proColon® compared to FIT. We describe the tradeoff relationship between low sensitivity and high false negative rate, leading to a harm of incorrectly telling a patient that they do not have cancer resulting in missing more cases of colorectal cancer when using Epi proColon®. Additionally, we show the tradeoff between low specificity and a high false positive rate, leading to the harm of incorrectly telling a patient that they have cancer when they do not, resulting in more unnecessary negative colonoscopies beyond FIT. We show that low test performance characteristics, i.e., sensitivity and specificity, can lead to high CRC screening test error rates, i.e., false positive and false negative test rates.
Epi proColon®
Comment: Many commenters expressed concerns that the currently available Epi proColon® test does not meet the criteria for an appropriate blood-based biomarker CRC screening test. One commenter suggested CMS reimburse Epi proColon® for three years until the test fulfills, in their opinion, the arbitrary performance values.
Response: We understand and appreciate the concerns regarding the Epi proColon® test. Based on the published studies and evidence reviewed, the Epi proColon® test does not meet test performance and health outcome criteria for a suitable and appropriate CRC screening test. Overall, we find that there is no direct or indirect evidence to support that routine screening for colorectal cancer with the blood-based Epi proColon® test will prevent cancer or improve mortality for the Medicare patients. We recognize the importance of an appropriate blood-based biomarker screening test and have established a pathway through this NCD for coverage of blood-based biomarker screening tests that meet the approved test criteria.
Approval Status
Comment: Many commenters expressed support for FDA authorization of blood-based biomarker screening tests. Several commenters believe that FDA authorization alone should be all that is necessary for Medicare coverage of such screening tests due to the FDA’s rigorous review process. One commenter expressed that requiring FDA authorization narrows patient access to clinically useful screening tests by eliminating a path for tests without FDA authorization. The commenter suggests that the NCD should include a coverage pathway for other tests such as those performed in a Clinical Laboratory Improvement Amendments (CLIA)-certified laboratory and those tests that voluntarily seek authorization by the FDA.
Response: We appreciate the supportive and suggestive comments. and agree that the FDA’s views are relevant in making decisions with respect to new colorectal cancer screening tests under section 1861(pp)(1)(D), but the statute does not make FDA’s views a controlling factor. Among other things, we are required to consult with appropriate organizations. We are maintaining FDA authorization as one requirement, not the sole requirement, for the approved blood-based biomarker CRC screening test. For cancer screening tests, FDA approval is important and provides the initial starting point for our review. CMS evaluates most importantly whether using the screening test improves survival in the general Medicare population (clinical utility). Patients who get tests that are not as good as other non-invasive stool-based screening may have early cancers that are missed and may receive more false positives and may undergo more diagnostic tests unnecessarily. MACs do not have authority to make coverage determinations with respect to expanding coverage for new colorectal cancer screening tests under section 1861(pp)(1)(D).
Comment: Two commenters suggested allowing Medicare Administrative Contractors (MAC) discretion for tests without FDA authorization.
Response: As explained above, the MACs do not have authority to make Medicare coverage determination on new colorectal cancer screening tests under section 1861(pp)(1)(D).
Comment: Several commenters encouraged CMS to cover FDA authorized blood-based biomarker screening tests based on the FDA’s indication for use. However, one commenter expressed that tests that are limited by their label to a subset of the screening population (e.g. patients that have declined all other guideline-recommended screening tests) would be difficult to enforce in clinical practice and potentially lead to inappropriate use.
Response: We appreciate the comments. We recognize the importance of the FDA label in clinical practice for safety and effectiveness. The final decision maintains the requirement for the blood-based biomarker test to have FDA market authorization with an indication for colorectal cancer screening along with the proven test performance characteristics, based on the pivotal studies included in the FDA labeling.
Testing Interval
Comment: Many commenters expressed concerns regarding the testing interval, specifically the option allowing FDA to indicate a specific testing interval. Many noted that FDA labeling typically does not set a specific testing interval, indicating that the FDA often requires completion of long-term post-approval studies before making any labeling recommendations on testing interval. Other commenters noted that the three-year testing interval was arbitrary and suggested alternate options for determining the testing interval including using the test developer’s data and relevant professional society guideline or consensus statement or the USPSTF recommendation.
Response: We appreciate these comments and removed the option to allow FDA to indicate a specific testing interval. We have adjusted the frequency interval for colorectal cancer screening with a blood-based biomarker test to once every 3 years with expedited adjustment if evidence supports such a change in the future. The rationale for this change is to maintain consistency with the past national coverage determination on a non-invasive colorectal cancer screening test based on similar evidence. The framework for the national coverage determination that approved the stool DNA screening test has evidence that supports a testing interval of once every 3 years. We removed the FDA determination of CRC screening test frequency from the decision language. Applying a similar framework to the blood-based biomarker test, the frequency of screening with a blood based colorectal cancer screening test will be once every three (3) years. A blood-based biomarker test meeting all of the NCD criteria will be assigned a three-year testing interval but we intend to consult with relevant professional society guideline or peer reviewed consensus statements and USPSTF recommendations and will adjust the frequency as appropriate in an expedited NCD for frequency only if evidence supports.
Patient Age Criteria
Comment: Multiple commenters noted that the American Cancer Society currently recommends that certain CRC screening modalities be initiated at 45 years of age and the draft USPSTF recommendation included a Grade B recommendation for CRC screening to begin at 45. They encouraged CMS to align its screening age requirements for all CRC screening tests.
Response: We appreciate the comments and will closely monitor professional organization recommendations on all CRC screening tests. Consistent with current existing professional organization recommendations and coverage of other CRC screening tests, we are finalizing the age range of 50-85 years. We recognize that there may be modifications and will closely monitor new evidence and recommendations. If the draft USPSTF recommendation is finalized and/or other society guidelines are revised, we may reconsider, in consultation with appropriate professional organizations, the appropriate CRC screening tests and address appropriately in an efficient manner. Due to the lower age, we believe the input of commercial insurers and other payers is also important since many individuals will have coverage through these other entities.
Comment: One commenter noted that their doctor told them that CRC screening is no longer done for patients over eighty.
Response: Medicare covers several colorectal cancer screening tests without restrictions due to age for patients over 80. Moreover, the USPSTF currently recommends the decision to screen for colorectal cancer in adults aged 76 to 85 years should be an individual one, taking into account the patient’s overall health and prior screening history.
Test Performance Criteria
Comment: The majority of commenters disagreed with setting a specific test performance threshold and many requested the removal of this requirement. Some had concerns that this would stifle innovation while others cited the specificity and sensitivity thresholds were arbitrary and not CMS’ role to determine. Many commenters offered a wide range of alternatives for performance criteria; including raising the sensitivity bar, clarifying the definition of specificity, modifying the sensitivity, utilizing CISNET microsimulation models, and adding performance criteria. Several commenters expressed concern with CMS using positive predictive value and stating indirect evidence did not exist.
Response: We appreciate the thoughtful comments, but we are not modifying the final decision to incorporate these changes. There is lack of strong high quality published evidence to support changing the specific cutpoints for point sensitivity and specificity. Given the inverse relationship between sensitivity and specificity, we could not provide an adequate rationale for altering the pre-specified cutpoints. If sensitivity was increased, then specificity would decrease for a screening test. If specificity was increased, then sensitivity would decrease. We felt that the pre-specified cutpoints allowed for a balance of the false positive rate against the false negative rate for the screening test. Thus, we believe that the pre-specified test performance characteristics would yield the most reasonable balance of the benefits and harms of the blood-based CRC screening test based on the limited evidentiary science available.
We also believe that having pre-specified test performance characteristics does not stifle innovation, and in fact promotes competition. We felt that having pre-specified cutpoints provides a targeted goal for manufacturers when they develop their blood based screening test. We think that competitive market forces will encourage manufacturers to develop screening tests with sensitivities and specificities above our minimum standard cutpoints. Competition in the commercial market place is likely to encourage subsequent iterations of blood based screening tests that would continue to improve upon test sensitivity and specificity.
In the Analysis section above on Harms of Lower Performance Screening for CRC Testing that was about screening test false positive and false negative rates, the discussion had a focus on screening test error rates. The purpose of this discussion was to describe the harms of the false positive and the false negative test result from a one-time screening using Epi proColon® compared to FIT. We describe the tradeoff relationship between low sensitivity and high false negative rate, leading to a harm of incorrectly telling a patient that they do not have cancer resulting in missing more cases of colorectal cancer when using Epi proColon®. Additionally, we show the tradeoff between low specificity and a high false positive rate, leading to the harm of incorrectly telling a patient that they have cancer when they do not, resulting in more unnecessary negative colonoscopies beyond FIT. We show that low test performance characteristics, i.e., sensitivity and specificity, can lead to high CRC screening test error rates, i.e., false positive and false negative test rates.
Adenoma Detection
Comment: Several commenters suggested the NCD should specifically address adenoma detection and should require a minimum performance for advanced adenoma detection.
Response: While we acknowledge the utility and potential clinical benefit of screening for advanced adenomas, there is very limited available evidence on the accuracy of blood-based tests to detect advanced adenomas and the sensitivity of FIT for advanced adenoma is low. Thus, we did not include point sensitivity or specificity to screen for advanced adenoma.
Decision Modeling Data
Comment: Many commenters were concerned that decision modeling studies, specifically Cancer Intervention and Surveillance Modeling Network (CISNET) microsimulation models were not included in the Evidence section and considered for the test performance criteria.
Response: We appreciate the comments and understand the concerns. While simulation modeling can be valuable tools that contribute to our understanding of colorectal cancer screening, there are challenges, such as uncertainty and USPSTFs approach, around the usefulness and applicability of modeling studies to blood-based biomarker testing for colorectal cancer screening. We included our assessment of the CISNET microsimulation models in the Analysis and discussed in detail why they did not meet the internal technology assessment criteria. There are challenges when considering the usefulness and applicability of modeling studies. For instance, it is unclear if modeling results should be considered on par with empiric evidence generated from studies on humans. How the USPSTF uses modeling studies should also be taken into consideration.
Guideline Inclusion
Comment: The majority of comments expressed concerns with the requirement for the blood-based biomarker screening test to be included as a recommended routine CRC screening test in at least one professional society guideline or consensus statement or USPSTF recommendation stating timing as a significant issue. It was noted that at the time of FDA authorization, the new test would not be included in any of these as standard of care and the process to update guidelines is often lengthy and not timely. Several commenters noted that Cologuard™ was not including in a guideline at the time of Medicare coverage. While most commenters requested the removal of this requirement, three commenters strongly supported guideline inclusion. A few commenters acknowledged that the Epi proColon® test was recently included in the National Comprehensive Cancer Network (NCCN) not for routine screening but for patients who refuse colonoscopy and stool testing.
Response: We appreciate the comments and understand the concerns regarding the timing involved with guideline inclusion so we have removed the requirement in the final decision. We continue to value the high standards involved in evidence-based guideline development and professional medical societies supporting the utility of a test. We understand and appreciate that this is a constantly evolving field. The draft USPSTF recommendation does not include other screening tests such as serum tests, urine tests, or capsule endoscopy because there is not yet enough evidence about the benefits and harms of these tests.
Follow-up Colonoscopy
Comment: Several commenters requested CMS clarify that colonoscopy performed as a follow-up to other initial non-invasive tests is part of the screening process and a covered preventive service.
Response: We appreciate the comments. We are actively working on Section 122 (Waiving Medicare coinsurance for certain colorectal cancer screening tests) of the Consolidated Appropriations Act 2021 and will revise using appropriate mechanisms.
Cost Effectiveness
Comment: Many commenters noted that blood-based biomarker screening tests could be more cost effective than currently approved Medicare CRC screening tests.
Response: We appreciate the comments regarding cost effectiveness. In general, for new colorectal cancer screening tests as noted in the background and analysis sections, we evaluate whether the test is appropriate. 42 C.F.R. § 410.37(a)(1)(v). We focus on whether the test prevents CRC and improves health outcomes in the Medicare population.
Clarifications
Comment: Two commenters were concerned that CMS had confused specificity with sensitivity regarding the section describing the clinical implications of low sensitivity. The commenters requested CMS review carefully to make sure the correct parameter is being discussed.
Response: The section on the clinical implications of low sensitivity was a discussion about the screening test error rates. Please see “Analysis on Sensitivity and Specificity” for the clarifying discussion around sensitivity and specificity.
Comment: One commenter requested we review and clarify the screening rates stated in the PDM.
Response: We appreciate the comment and have revised the language in the Background and Analysis sections to include “adults who were up to date with” CRC screening tests had a percentage of 79.2% for individuals aged 65 to 75 years old.
Comment: Another commenter cited the Johnson 2014 study and stated that they believed we incorrectly stated the detection rates for Epi proColon® and FIT in the PDM.
Response: We appreciate the comment and reviewed the citation to confirm that study is cited correctly.
VIII. CMS Analysis
National coverage determinations are determinations by the Secretary with respect to whether or not a particular item or service is covered nationally by Medicare (§1862(l) of the Act). Among other things, in order to be covered by Medicare, an item or service must fall within one or more benefit categories contained within Part A or Part B, and must not be otherwise excluded from coverage. CRC screening tests have a benefit category under §1832, §1861(s)(2)(R) and §1861(pp) of the Act. Specifically, CMS is using the authority under section 1861(pp)(1)(D) and 42 CFR 410.37(a)(1)(v) to determine whether the scope of the CRC screening benefit should be expanded to include coverage of blood-based biomarker tests.
Due to the natural history of colorectal neoplasia, the burden of CRC and large pre-cancerous adenomas is high in older adults. In this analysis, we will evaluate specific criteria of screening tests as described by Cochrane and Holland (1971) and noted in the introductory paragraphs of the evidence (See section VII of this decision memorandum), in addition to the hierarchical framework of Fryback and Thornbury (1991).
We will adapt the hierarchical framework of Fryback and Thornbury (1991) in our analysis of blood-based biomarker screening tests for colorectal cancer. We will look for sound evidence that shows the screening test is analytically and clinically valid (Levels 1-2), since there is no direct evidence on clinical utility that shows that blood-based colorectal cancer screening tests improves health outcomes, such as mortality or cancer survival, to benefit Medicare beneficiaries.
As Cochrane and Holland (1971) noted, “evidence on health outcomes, for example, evidence that screening can alter the natural history of disease in a significant proportion of those screened," is important in the consideration of screening tests since individuals are asymptomatic and "the practitioner initiates screening procedures." Since a number of colorectal cancer screening tests are available and covered by Medicare, how a new test should be used and how it fits into current recommendations for screening should also be considered when determining whether a new test is appropriate. We used this approach in the decision memo on Screening for Colorectal Cancer - Stool DNA Testing (CAG-00440N).
Appropriate CRC Screening Tests
Our approach to determine which CRC screening tests are appropriate to include in the Medicare program was first used in the NCD on screening fecal immunochemical tests. We applied this same approach to the NCD on screening stool DNA tests. We will apply the same approach to blood-based biomarker screening tests. In the past CRC screening NCDs, we have discussed appropriate test performance criteria such as point sensitivity and specificity compared to colonoscopy. We note that the determination of appropriateness is similar to the consideration of what is appropriate for the device to be, “at least as beneficial as an existing and available medically appropriate alternative.”
Through the evaluation of evidence from published studies, the clinical data for the device must reach the threshold for being appropriate. The direct evidence by Shaukat, et al. (2013) and Levin et al. (2018) suggests that there is clinical utility in using FOBT and FIT for early detection of colorectal cancer (CRC) because these tests reduce mortality of the disease. Conversely, there is no direct evidence on outcomes such as mortality for blood-based biomarker tests used in screening for colorectal cancer. Therefore, we assessed whether there was supporting indirect evidence from studies that used gFOBT or FIT as comparators to establish a link to the screening test under consideration. By comparing the test performance characteristics, defined as sensitivity, specificity, and positive predictive value, of new screening tests to gFOBT or FIT, we can assess whether blood-based tests might translate into similar reductions in disease mortality for Medicare beneficiaries. Thus, if the sensitivity and specificity of the new screening tests are as good as or better than the sensitivity and specificity of gFOBT or FIT, then we have indirect evidence suggesting that the new blood-based biomarker tests may reduce colorectal cancer mortality.
The FDA suggested a similar approach. In FDA’s review of the in vitro diagnostic device Epi proColon® under the premarket approval (PMA) process, the FDA stated that “to appropriately define test performance, it is important to evaluate the disease spectrum representative of the screening population. FDA has suggested that a cross-sectional clinical study supporting the performance of an in vitro diagnostic device for CRC screening be designed in the context of fecal immunochemical test (FIT) performance. FIT is a recommended screening modality across different guidelines. [Guaiac] [f]ecal occult blood test (gFOBT) screening is supported by long-term longitudinal follow-up (Shaukat A, 2013). Additionally, since different studies have reported a range of FIT performance [references], a direct head-to-head comparison to a FIT assay with well-documented CRC screening experience in the intended use setting is warranted to assess the performance of a new in vitro diagnostic device.” (FDA, Epi proColon® FDA Executive Summary, March 26, 2014).
The American Cancer Society also suggested a similar “evidence based inferential reasoning” methodology. In the 2018 colorectal cancer screening guideline update, the ACS reported that “[r]esults from randomized controlled trials (RCTs) of CRC screening with either a stool-based test (gFOBT) or a structural examination (flexible sigmoidoscopy [FS]) have demonstrated mortality reductions associated with the detection of advanced neoplasia in asymptomatic adults.26 The evidence of benefit for all other screening tests is limited to test performance data demonstrating the ability to detect early stage CRC and/or advanced adenomas and observational studies. In addition to this body of evidence for the individual modalities, the GDG [Guideline Development Group] adopted evidence-based inferential reasoning to extrapolate from the evidence establishing a rationale for using the detection of occult blood as an effective screening tool to support fecal immunochemical testing (FIT) and multitarget stool DNA (mt-sDNA) testing, which includes multiple molecular assays combined with a hemoglobin immunoassay.” (Wolf, 2018)
Test Performance Characteristics
As suggested by Cochrane and Holland (1971), test performance characteristics are defined as sensitivity and specificity. We also include positive predictive value as a test performance characteristic.
However, the validation of a screening test does not include an assessment of adherence or compliance with CRC screening guidelines (Cochrane and Holland, 1971). Level 2 diagnostic accuracy efficacy, or test performance characteristics, is defined as sensitivity and specificity in a defined clinical problem setting, not compliance with screening guidelines (Fryback, 1991). Adherence can be measured as participation rates in an organized screening program that complies with a set of CRC screening guidelines or uptake of a screening test (D’Andrea, 2020; Liles, 2017). Adherence or compliance with CRC screening guidelines should not be considered a test performance characteristic of a screening test. In this Analysis, test performance characteristics to evaluate the benefit of a blood-based CRC screening test are sensitivity, specificity, and positive predictive value, but not adherence.
Clinical Utility versus Clinical Validity
The comparative studies fail to show clinical utility of Epi proColon® as a blood-based CRC screening test, given the lack of direct or indirect mortality data. Sensitivity, specificity, and positive predictive value measure the accuracy of the test to assess clinical validity of the test. These outcomes assess the ability of the test to accurately identify colorectal cancer in patients screened for cancer. Sensitivity and specificity do not provide direct evidence on net health outcomes. Mortality is direct evidence of the net health outcome of the CRC screening test. Mortality, or survival, measures the impact of the screening test on health outcomes to assess clinical utility of the test and is dependent on the detection of large adenomas and early stage cancer where treatments have been shown to be more effective. Mortality is a health outcome relevant to Medicare beneficiaries being screened for colorectal cancer. These comparative studies fail to show clinical utility of Epi proColon® as a screening test to detect methylated SEPT9 DNA levels because mortality is not measured. There is insufficient information due to the lack of mortality data to assess the direct evidence of the clinical utility for the blood-based Epi proColon® screening test on health outcomes, such as mortality, in Medicare beneficiaries.
Question 1: Is the evidence sufficient to determine that a blood-based biomarker test (at the time of this review Epi proColon® is the only FDA approved commercially available blood-based biomarker screening test) is an appropriate colorectal cancer screening test for prevention or early detection in Medicare beneficiaries?
No, the evidence (direct or indirect) does not demonstrate that screening in Medicare beneficiaries using the Epi proColon® test is suitable for prevention or early detection of colorectal cancer. The published evidence does not show that the available blood-based biomarker CRC screening test improves health outcomes for Medicare beneficiaries. The indirect evidence (comparing a blood-based screening test to another test that has been shown to improve mortality such as screening fecal immunochemical test) does not show that blood-based screening test is equivalent in the detection of large adenomas or early stage cancer. The test performance of the Epi proColon® test does not meet sensitivity and specificity levels established by prior evidence at which the benefits of using the screening test outweigh harms to Medicare patients. To provide clarity to innovators and to reduce burden of a reconsideration of this NCD, we provide a direct pathway for coverage of blood-based biomarker CRC screening tests when the criteria are met.
As noted above, the detection of large adenomas is important to prevent development of CRC. The detection of early stage cancer when treatments are most effective is important in achieving improved survival. Four meta analyses and 15 comparative studies provided evidence for this analysis. All of the published studies, except for one study (Yang, 2019) which examined progression free survival, used test performance (sensitivity and specificity) as the outcome to assess the performance of Epi proColon® as a screening test for colorectal cancer.
Test performance characteristics, defined as sensitivity and specificity, varied depending on where the study was located. The test performance characteristics of the SEPT9 assay in the Asian population might be different from that of other races, largely driven by differences in study design methodologies, although geographic variability can be a proxy for other factors. Song, Jia, Yu, et al. (2017) speculated that the differences in the test performance characteristics “might be due to the
use of different SEPT9 assays or the difference between average-risk and high-risk population… The kits used and the population involved were quite different. Epi proColon® assay was the test kit in PRESEPT study while Epi proColon® 2.0 CE assay was used in this study. The PRESEPT study focused on the average-risk population while this study focused on the high-risk population from hospitals…Therefore, whether there is a difference between Chinese and other ethnicities needs further investigation under identical study setting.” Hu et al. (2019) “found that the diagnostic sensitivity increased in patients of Asian ethnicity compared to those of white ethnicity (p=0.04), indicating that the diagnostic value of mSEPT9 varies by ethnicity.” The Hu (2019) study authors did not opine on the underlying reason for their findings.
In a meta-analysis by Hariharan et al. (2020), specificity reported for Asian countries was different when compared to North America. Hariharan, et al. (2020) found that “[t]here was some evidence that the threshold [1/3 or 2/3 algorithm, with positive test result defined as one or two positive findings out of three runs] used contributed to the heterogeneity of Asian studies (Spearman’s coefficient 0.793, p=0.02), but no such evidence was observed for European or North American studies or large or small studies…. There was strong evidence (p<0.01) that the heterogeneity in specificity was largely affected by size of study, and whether it was conducted in Asian (p<0.01) or North American (p<0.001) regions.” The authors concluded that “[p]revious meta- analyses reported that estimates of sensitivity and specificity were highly heterogeneous, probably due to differences in test performance by geographic region of recruitment of participants. [They] also observed marginal evidence that some of heterogeneity could be due to varying ctDNA positivity thresholds inferring that test accuracy depended on the positivity algorithm, with the optimum threshold level being the 2/3 algorithm. The North American studies had overall lower pooled diagnostic accuracy indicators potentially due to different positivity threshold used in that region. As reported by Nian et al,4 [they] found marginal evidence for the sensitivity being lower for studies with a higher proportion of early stage disease is expected given earlier stage CRC would be expected to produce lower amounts of circulating mSEPT9 given fewer cancer cells at the site of the original tumour and no metastases” (Hariharan, 2020). However, the evaluation of colorectal cancer stage was not stratified by race or geographic location of the study, precluding any exploration of an underlying biological mechanism to account for the differences in test performance characteristics. The evidence is insufficient to assess other potential proxy factors such as biological or environmental mechanisms. The evidence suggests that the test performance characteristics of the SEPT9 assay in the Asian population might be different from that of other races, and may likely result from differences in study design methodologies applied across studies conducted in varying geographic locations, rather than a biological mechanism.
In stratified analyses by population subgroup, among a no evidence of disease group, the Chinese population showed no statistical difference in false positive rate compared to the Caucasian population that was at least 50 years-old (Song, Jia, Yu, 2017). Conversely, a statistically significant difference in the false positive detection rate was observed between the Chinese and African American population in the 50–59 year-old age group (Song, Jia, Yu, 2017). The results of the PRESEPT study found specificity correlated with being African American, though the study included White and African American participants and not Asian participants (Potter, 2014). In a different study, there was no statistically significant impact of race on specificity, with race defined as Black, Caucasian, and Hispanic, with the study not including Asians (Johnson, 2014). Sensitivity was higher among Asian patients when compared to Caucasian patients (Hu, 2019). The Yang (2019) study indicated “[p]revious studies found that the incidence of CRC and the sensitivity to the mSEPT9 test assay in different ethnic groups were different.” Because the specificity and sensitivity of Epi proColon® appears to have differing performance characteristics for people of Asian ethnicity, the generalizability of studies conducted entirely in an Asian population might not be broadly applicable to the U.S. population for assessing benefits of CRC screening. Thus, studies of Asian populations are not representative of the United States and are not generalizable to the Medicare population. Studies conducted in Asian countries are excluded from the Analysis; we will stress U.S. based evidence more heavily in our analysis of blood-based CRC screening tests due to generalizability to the Medicare population.
Across the comparative studies in the United States, the performance of the Epi proColon® test varied. From the comparative studies, a summary of test performance characteristics is presented in Table 1 below.
In Table 1, of the four clinical research studies (Church, 2014; Johnson, 2014; Potter, 2014; Warren, 2011) located in the United States, one study (Church, 2014) used an earlier first generation Epi proColon® assay and the other study (Warren, 2011) used the PCR method to test for mSEPT9 DNA. The Church et al. (2014) study enrolled participants in the PRESEPT study population. The PRESEPT study was a prospective study comprised of average risk, asymptomatic individuals ≥50 years old scheduled to undergo screening colonoscopy at 32 US (22) and German (10) clinical centers and who voluntarily gave blood plasma samples before colon preparation. The Church et al. (2014) study used the first generation Epi proColon® Assay (Epigenomics AG, Berlin, Germany), and the study population consisted of 7941 men (45%) and women (55%), who had a mean age 60 years enrolled from June 2008 until January 2010. Among the 53 CRC cases and 1457 subjects without CRC, the sensitivity of mSEPT9 for detecting colorectal cancer was 48.2%, which is below the sensitivity (68%) for the Potter (2014) study. Specificity was 91.5%, which is above the specificity (80%) for the Potter (2014) study.
Samples from this same patient population used by Church and colleagues were later used by Potter and colleagues who accessed the archived prospectively collected plasma samples from the PRESEPT clinical trial. But Potter and colleagues used a subsequent generation test — the Epi proColon® test comprised of the Epi pro-Colon® Plasma Quick kit, PCR kit, and Control kit. Because these two U.S. studies (Church, 2014; Potter, 2014), are two sequential studies involving samples from the same patient population and applying two superseding generations of Epi proColon® tests, this analysis references the initial test conducted by Church et. al., (2014) but will focus on the applicability of the study conducted by Potter et al., (2014) that used the only U.S. FDA market-authorized test among the two that is now available in the US. However, both first and second generation blood-based tests used one biomarker, mSEPT9 which may be the overall bounding factor on test performance for CRC and advanced adenomas.
The case-control study by Warren (2011) collected plasma samples from 50 untreated CRC patients at one U.S. and two Russian institutions, and 94 control samples from CRC-free patients at four U.S. institutions within one year of having a negative colonoscopy. This study used a SEPT9 methylated DNA test (with PCR amplification performed in triplicate for each sample) and “using a modified version of the protocol from deVos et al.” The test was developed by the investigators (ARUP Laboratories, Inc., a non-profit national reference laboratory, from the University of Utah and its Department of Pathology) to try to improve upon the first generation Epi proColon® test. The authors reported that the “test had an overall sensitivity for CRC of 90.0%”, which is above the sensitivity (68%) of the Potter (2014) study. The specificity was 88.3% for detecting CRC in patients of all stages, which is above the specificity (80%) of the Potter (2014) study. “In the small prospective cohort study, the SEPT9 test detected 12% of adenomas with a false-positive rate of 3%.” While the test results reported by Warren et. al were promising, it does not appear that the investigators pursued an FDA market authorized test that might be available to U.S. Medicare beneficiaries. Therefore, while intriguing, the data from this one study involving a non–FDA market-authorized test are not particularly informative to the current NCD consideration.
Therefore, of the four U.S. studies in Table 1 (Church, 2014; Johnson, 2014; Potter, 2014; Warren, 2011), the preponderance of discussion in this NCD analysis will center on the Johnson (2014) and Potter (2014) studies. The study by Warren (2011) will not be discussed further in this section of the Analysis because of use of a non-FDA market authorized test. The sample size of the Warren (2011) study was small, which is a major limitation of this study that can lead to an erroneous conclusion being drawn from the study. The overall test performance characteristics for the Church (2014) study are lower than that of the Potter (2014) study, such that its inclusion in the analysis would lead to lower estimate of Epi proColon’s test performance characteristics. Since versions in both studies tested for mSEPT9, the increase in sensitivity coupled with a decrease in specificity in the study by Potter et al. from the study by Church et al. suggest adjustments in the analytic algorithm and cutoff points for calling positive and negative tests. Because the test kits have differences in FDA marketing status, most of the discussion in this analysis will center on the Johnson (2014) and Potter (2014) studies.
A full table of the sensitivity and specificity of all of the comparative studies found in our literature search is listed in Table 4a Appendix D. The other studies in Table 4a beyond the listing in Table 1 were conducted outside of the United States, thus the remaining study results outside of Table 1 might not be generalizable to the Medicare population due to geographic variability.
Table 1. Sensitivity and Specificity of Comparative Studies in the United States |
| |
Sensitivity (95% CI), % |
P value |
Specificity (95% CI), %, |
P value |
|
Colorectal cancer |
Advanced adenoma-precancerous lesions |
|
Colorectal cancer free |
|
| Church, 2014 |
|
|
|
|
|
| Epi proColon® |
48.2 (32.4- 63.6) |
11.2 (7.2-15.7) |
|
91.5 (89.7-93.1) |
|
Johnson, 2014 |
|
|
|
|
|
| Epi proColon® |
72.2 (62.5–80.1) |
|
> 0.05 |
80.8 (74.7-85.8) |
< 0.05 |
| FIT |
68.0 (58.2–76.5) |
|
|
97.4 (94.1-98.9) |
|
Potter, 2014 |
|
|
|
|
|
| Epi proColon® |
68 (53–80) |
22 (18–24) |
|
80.0 (78–82) |
|
Warren, 2011 |
|
|
|
|
|
| Epi proColon® |
90.0 (77.4-96.3) |
|
|
88.3 (79.6- 93.7) |
|
In the retrospective study from the pivotal prospective PRESEPT clinical trial, Potter et al. (2014) found that the point sensitivity for all stages of CRC was 68% and that point specificity, based on negative colonoscopy findings, was 80.0%, when adjusted to the PRESEPT cohort. In a prospective cohort multicenter study, Johnson et al. (2014) reported a slightly higher sensitivity than Potter et al. (2014) but a similar specificity.
For the pivotal PRESEPT clinical trial conducted in an average risk population, sensitivity was “within the expected range and within the defined specifications” (Epigenomics AG, Summary of Safety and Effectiveness Data [SSED] Epi proColon® March 26, 2014). But at the FDA panel review of Epi proColon® on March 26, 2014, it was reported that “[t]he pivotal clinical study [Potter, 2014] [did] not meet all of the pre-specified primary performance objectives” (FDA, Epi proColon® FDA Executive Summary, March 26, 2014). “The test showed lower specificity results than had been required by the Design Input Requirement” (Epigenomics AG, Summary of Safety and Effectiveness Data [SSED] Epi proColon®. March 26, 2014). In the non-CRC group (comprised of AA [advanced adenoma], SP [small polyps], and NED [no evidence of disease]), specificity did “not meet the criterion that Epi proColon® shall demonstrate specificity of 85%. The false positive rate of 21% is higher than expected, indicating that more individuals (than expected) will be recommended to undergo a follow-up diagnostic procedure, such as colonoscopy, which will be negative.” (FDA, Epi proColon® FDA Executive Summary, March 26, 2014). “The lower specificity leads to the potential for an increase in avoidable negative diagnostic colonoscopies and colonoscopy-related adverse events” (FDA, Epi proColon® FDA Executive Summary, March 26, 2014). Further, “[s]ome Panel members stated that sensitivity of the test is not adequate for a first-line screening test; others noted that the specificity is not adequate for a screening test” (FDA, 24 Hour Brief Summary, March 26, 2014).
At the FDA panel review of Epi proColon® on March 26, 2014, in the pivotal PRESEPT clinical study by Potter et al. (2014), it was reported that “specificity was sensitive to age” (Epigenomics AG, Executive Summary: Product Summary and Briefing Packet Epi proColon®. March 26, 2014). “There is evidence of a decrease in specificity of Epi proColon® with increasing age, as observed with the increasing false positive detection fractions (PDFs) with increasing age groups in non-CRC subjects” (FDA, Epi proColon® FDA Executive Summary, March 26, 2014). “The increase in PDF values in subjects over 69 years of age has been attributed to age-related increase in methylation as described in the literature” (Epigenomics AG, Summary of Safety and Effectiveness Data [SSED] Epi proColon® March 26, 2014). “However, the clinical studies were not designed to assess test performance in subgroups, so those analyses should be interpreted with caution” (FDA, Epi proColon® Transcript, March 26, 2014). But “[f]or age, the Panel agreed that a warning should be included in the labeling to inform users that the test has a higher false positive rate in the older (above age 75 years) population” (FDA, 24 Hour Brief Summary, March 26, 2014).
Our analysis focused on the point estimates for sensitivity and specificity, and not the upper and lower bounds of the 95% confidence interval. We believe that there is much uncertainty surrounding the upper and lower bounds of the 95% confidence interval which is strongly affected by the sample size of the study population. A study with a small sample size will have a wide confidence interval due to the large degree of uncertainty around the variability of the point estimates for sensitivity and specificity compared to a study with a large sample size. A study with a large sample size has a more precise point estimate of sensitivity and specificity and thus, a narrow confidence interval with the upper and lower bound closer to the point estimate. Our analysis compares point estimates, and not the upper and lower bounds of the confidence interval.
The clinical implications of low specificity for a CRC screening test is missing individuals with colorectal cancer. Low specificity increases the false negative rate leading to a negative screening test result for an individual with colorectal cancer. The individual who has a follow up diagnostic colonoscopy could be positive for colorectal cancer, despite having a negative CRC screening test. Thus, a person with colorectal cancer will be missed since the screening test was incorrectly negative.
Because the Epi proColon® test showed a point specificity below its pre-specified test performance criterion, the pivotal PRESEPT clinical trial (Potter, 2014) did not meet all of the primary test performance objectives.
Table 2. Sensitivity and Specificity of Epi procolon® versus FIT or gFOBT in US Studies |
|
Sensitivity % (95% CI) |
P-value |
| Colorectal Cancer |
Comparative study |
|
Epi proColon® 2.0 |
FIT |
|
Johnson, 2014 (n=97) |
72.2 (62.5–80.1) |
68.0 (58.2–76.5) |
>0.05 |
|
Specificity % (95% CI) |
|
| Colorectal Cancer Free |
P-value |
Comparative study |
|
Epi proColon® 2.0 |
FIT |
|
Johnson, 2014 (n=193) |
80.8 (74.7-85.8) |
97.4 (94.1-98.9) |
<0.05 |
* Two non US studies (Sun, 2019; Tóth, 2012) compared Epi proColon® to FOBT/gFOBT (see Table 4a, Appendix D).
As shown in Table 2, when the Epi proColon® test was compared to FIT test using colonoscopy as the reference method for detection of CRC, the Johnson study (2014) found the Epi proColon® test to be statistically non-inferior to the FIT test with respect to sensitivity but it did not achieve non-inferiority for specificity, with somewhat wide confidence intervals. For specificity, the difference between tests was 16.6% in favor of FIT. These results indicate “that the Epi proColon® test exhibited a higher rate of false positive results compared to the FIT test” (Epigenomics AG, Summary of Safety and Effectiveness Data [SSED] Epi proColon® March 26, 2014). At the FDA panel review of Epi proColon® on March 26, 2014, it was reported that “as compared to the FIT test used in the study, the lower specificity for Epi proColon® leads to the potential for a relative increase in avoidable colonoscopies and the adverse events associated with colonoscopies” (FDA, Epi proColon® FDA Executive Summary, March 26, 2014). “Additionally, there is no statistically significant sensitivity benefit of Epi proColon® relative to FIT. Thus, there is uncertainty as to whether Epi proColon® is an appropriate substitute for CRC screening options such as FIT” (FDA, Epi proColon® FDA Executive Summary, March 26, 2014).
For test performance characteristics, point sensitivity of Epi proColon® is no better than FIT in detection of colorectal cancer. As compared to the FIT test, the point specificity for Epi proColon® was lower (97.4% versus 80.8%, respectively). There is no evidence that shows screening for colorectal cancer with Epi proColon® is more effective than FIT. Compared to FIT, there is no indirect evidence that using Epi proColon® is as effective for colorectal cancer screening among Medicare beneficiaries.
Advanced Adenoma
| Table 3. Sensitivity of Advanced Adenoma (U.S. studies) |
|
Sensitivity (95% CI), % |
Sample Size (n) |
|
Colorectal cancer |
Advanced adenoma-precancerous lesions |
|
Church, 2014 |
|
|
|
| Epi proColon® |
48.2 (32.4- 63.6) |
11.2 (7.2-15.7) |
314 |
Potter, 2014 |
|
|
|
| Epi proColon® |
68 (53–80) |
22 (18–24) |
621 |
As shown in Table 3, compared to colorectal cancer, the sensitivity for advanced adenoma of the blood-based tests based on mSEPT9 were lower (point estimates of 11.2% and 22%). No prospective study has reported the sensitivity of the second generation Epi proColon® test for advanced adenomas. Additional research is needed. The ability of a CRC screening test to detect advanced adenomas is essential to prevent cancer by removing the adenoma before it progresses and is one advantage to direct visualization tests like screening colonoscopy. Of the non-invasive tests, the stool DNA test (Cologuard®) had a sensitivity of 42.4% for advanced adenomas (Imperiale, 2014) and FIT had a sensitivity of 27% for advanced adenomas (Niedermaier, 2017).
Age Range
Several studies assessed the relationship between test performance characteristics of sensitivity and specificity against age. In a study located predominately in the US, decreasing specificity was found to be correlated with increasing age and appeared to plateau above at least 60 years of age, but there was no statistical testing of age categories shown in the results (Potter, 2014). There was “some variation in the positive detected fraction for non-CRC subjects based on age, with the highest fraction for subjects in the 60–69 [year old] class”, but the effect was not statistically significant (Johnson, 2014). The authors of the Johnson (2014) study concluded that there was no significant differences in specificity or sensitivity with respect to age in the U.S. population. The evidence suggests that there might be a trend indicating variation in specificity above at least age 60 years, even though it is not statistically significant. The evidence from the published literature for the relationship of sensitivity and specificity against age is inconsistent, but age might have an adverse effect on the test performance characteristics of the blood-based CRC screening test, especially over the age of 65 years. Epi pro Colon® instructions for use state that “The rate of false positive Epi proColon® results increases with age. Test results should be interpreted with caution in elderly patients. See Performance Characteristics in Section 13.” (Epigenomics AG, Instructions for Use [IFU] Epi proColon®. March 26, 2014.) The evidence for the impact of test performance on age is uncertain, thus, more research is needed to identify potential starting and stopping age for blood-based CRC screening in the Medicare population.
Study Limitations
These comparative studies had several limitations. One limitation of one of the studies is the presence of a small sample size (Church, 2014). Small sample sizes in the cited studies led to wide confidence intervals for specificity and sensitivity and a greater variability in the estimate of the sensitivity and specificity of the Epi proColon® test. Chance variability in the relationship between the use of Epi proColon® and its sensitivity and specificity may have accounted for the results observed in any individual study. Because of chance, the study results may have overestimated or underestimated the true sensitivity and specificity of Epi proColon® as a screening test. This could lead to an imprecise effect estimate of the performance of the Epi proColon® test, lack of robust data, and an invalid conclusion being drawn from the results of these studies.
Other limitations are that all 19 of the published comparative studies reviewed were observational studies. While analytic observational studies with a control group (such as case-control studies) help in understanding the risk/benefit profile of interventions, they lack randomization that can help to control bias. Evidence from observational studies is more likely to be subjected to bias than from a randomized controlled trial, the highest level of evidence. There are no randomized clinical trials of blood-based CRC screening tests. Bias, or systematic error, is an issue in the design or conduct of a study that can introduce distortions in observed relationships between an exposure and an outcome; in this case, use of Epi proColon® as a screening test, and an outcome measure such as sensitivity, specificity, or mortality. This could lead to invalid inferences that could overestimate or underestimate the test performance characteristics of Epi proColon® as a screening test for colorectal cancer.
Another limitation of the cited studies is the retrospective nature of several studies (Potter, 2014; Warren, 2011). Bias might not be entirely minimized a priori in the design of these studies. For example, there might be bias from not systematically collecting all the data, such as sociodemographic data, from all of the patients. Thus, selection bias due to missing data could alter any conclusions drawn from the study.
One study (Warren, 2011) was a case control study. A major limitation of a case control study is selection bias, where presence or absence of an exposure may influence which particular diseased CRC cases or non-diseased individuals are enrolled in the study. This can result in the CRC cases not being comparable to the non-CRC controls and thus, the controls not being selected from the same study population as the CRC cases. This can result in the non-CRC control group not being truly representative of the population that produced the CRC cases. Lack of comparability between CRC cases and non-CRC controls might distort any conclusions drawn from the study results.
Meta Analyses
Across the four meta analyses which selected US and non US based studies (Hariharan, 2020; Hu, 2019; Song, Jia, Peng, et al. 2017; Yan, 2016), different types of assays were used in the studies. Both generations of the Epi proColon® test were used, along with other different test kits for mSEPT9. Other mSEPT9 test kits included laboratory developed tests (LDTs), research kits and the SensiColon assay, with none of the other test kits approved by the FDA. The SensiColon assay for blood samples was approved by the Chinese FDA (Song, 2016), but has not been approved by the US FDA. The meta analyses integrated both US FDA approved and non US FDA approved assays. Collective results were not stratified by type of SEPT9 DNA test type. Because the focus of this NCD is on US FDA approved assays, the collective data/findings that integrated non US FDA approved assays were excluded from the Analysis. Another limitation is that two meta-analyses (Hu, 2019; Song, Jia, Peng, et al., 2017) showed heterogeneity in the studies selected for inclusion. Hariharan et al. (2020) reported considerable heterogeneity in the pooled estimates for both sensitivity and specificity. Across the studies selected for the meta analyses, some were located in the U.S., while many others were in Europe, Southeast Asia and China, raising the concern of geographic variability. Lack of comparability across the studies included in the meta-analyses is likely to distort any conclusions drawn from the meta-analysis results. Therefore, the four meta analyses (Hariharan, 2020; Hu, 2019; Song, Jia, Peng, et al. 2017; Yan, 2016) contribute to our broad understanding but will not be further discussed in this Analysis.
Overall, the Epi proColon® test is not a suitable screening test for CRC. There is no direct evidence that shows screening for colorectal cancer with Epi proColon® is more effective than FIT. Observational studies measuring sensitivity and specificity, which are indicators of clinical validity, demonstrated that sensitivity of Epi proColon® is no better than FIT in detection of colorectal cancer. As compared to the FIT test, the specificity for Epi proColon® was lower. Therefore, compared to FIT, there is no indirect evidence that using the blood-based Epi proColon® test is appropriate for prevention or early detection of colorectal cancer among Medicare beneficiaries. This is consistent with the USPSTF (USPSTF, 2016), the United States Multi-Society Task Force (Rex, 2017), the ACS (Wolf, 2018), and the NCCN (NCCN, 2019; NCCN, 2020) who do not recommend using Epi proColon® to routinely screen patients for colorectal cancer.
Question 2: Is the evidence sufficient to determine that colorectal cancer screening using a blood-based biomarker screening test is appropriate for Medicare beneficiaries?
No, the published evidence does not demonstrate that the available blood-based biomarker screening test will prevent progression of advanced adenomas to cancer or improve health outcomes for patients found to have colorectal cancer. To provide clarity to innovators and to reduce burden of a reconsideration of this NCD, we provide a direct pathway for coverage of appropriate blood-based biomarker CRC screening tests when the criteria are met.
Among the cited studies, the study populations had a mean age between 55 and 71 years, and for persons at least age 60 years old, the percent ranged from 35.8% to 76%. Both genders were adequately represented in the evidence base. Even though the study populations were relatively balanced, some were slightly in favor of women (Church, 2014; Ørntoft, 2015; Sun, 2019). Epi pro Colon® instructions for use state that “The rate of false positive Epi proColon® results increases with age. Test results should be interpreted with caution in elderly patients. See Performance Characteristics in Section 13.” (Epigenomics AG, Instructions for Use [IFU] Epi proColon®. March 26, 2014.)
While some of the clinical research studies were conducted in the United States (4 studies), many studies were completed in Europe (4), China (8), and Russia (1). This includes two studies enrolling patients in both the U.S. and Germany (Church, 2014; Potter 2014) and one in both the US and Russia (Warren, 2011). One study (Hitchins, 2019) did not identify the location of its study site. The majority populations were Caucasian (Johnson, 2014; Ørntoft,2015; Potter, 2014; Tóth, 2012) or Chinese (He, 2018; Jin, 2015; Song, 2016; Song, Jia, Yu, et al., 2017; Song, Peng, Li, et al. 2017; Song, 2018; Sun, 2019; Yang, 2019). There is geographic variability which might reflect differences in the medical care systems and how screening is implemented, or differences in study design methodologies as applied in different geographic locations. The findings from these studies conducted outside the US might not be directly applicable to the Medicare population. Thus, some studies might not be entirely relevant in generalizations of the results to the Medicare population.
CRC Screening Approaches
At this time, no professional society recommends any blood-based biomarker test for CRC screening. The USPSTF has not included a blood-based biomarker test as a recommended option in their CRC screening recommendation. While we recognize the importance of FDA approval of CRC screening tests, the FDA indication for use for Epi proColon®, the only commercially available blood-based biomarker test in the US at this time, is limited in scope and not indicated as a routine screening test for the general population. Consistent with past CRC screening NCDs, there are no appropriate professional organizations such as the USPSTF, the U.S. Multi-Society Task Force, the American College of Gastroenterology, the American Cancer Society, and the National Comprehensive Cancer Network that have recommended a blood-based biomarker screening test in published guidelines or consensus statements.
A number of professional societies and organizations have developed guidelines for CRC screening, although some of the details of the recommendations differ. There is agreement in that the organizations recommend against using Epi proColon® to routinely screen patients for colorectal cancer. The USPSTF (USPSTF, 2016) found the SEPT9 DNA test to have low sensitivity for detecting colorectal cancer and, therefore it was not included in a menu of options as a strategy for colorectal cancer screening. The U.S. Multi-Society Task Force of Colorectal Cancer (MSTF; Rex, 2017), which represents the American College of Gastroenterology, the American Gastroenterological Association, and The American Society for Gastrointestinal Endoscopy, suggests that the Septin9 serum assay (Epigenomics, Seattle, Wash) not be used for screening (weak recommendation, low-quality evidence). The NCCN (2019) does not recommend the SEPT9 DNA test in routine screening for colorectal cancer. The ACS (Wolf, 2018) concluded that given the limitations in the methylated Sept9 test, they decided to not have the test among the list of recommended routine CRC screening options for average-risk adults (Wolf, 2018).
The 2020 NCCN colorectal cancer screening guidelines indicate that the mSEPT9 blood test is not recommended for routine screening, “but may provide an alternative for individuals who refuse other screening modalities” (NCCN, 2020). The NCCN guidelines also reports one factor that may potentially negatively impact the performance of the SEPT9 DNA test is age > 65 years (NCCN, 2020). Since the mSEPT9 test appears as a footnote underneath the screening modality and schedule algorithm diagram, it is unclear if the test performance for mSEPT9 test is considered on par with the test performance for high-sensitivity guaiac-based or immunochemical-based testing or FIT-DNA-based testing. Thus, it is uncertain if the mSEPT9 test is considered a part of the menu of choices as an alternative to the recommended fecal-based tests, i.e., gFOBT or FIT, in routine screening for colorectal cancer. Also the NCCN guidelines list the mSEPT9 test as an “emerging option” for CRC screening (NCCN, 2020). The NCCN guidelines do not discuss sensitivity or specificity of the mSEPT9 test, thus, the evidence is insufficient to assess if the test performance characteristics of the mSEPT9 test is as good as that of FIT. The 2020 NCCN guidelines do not show evidence to recommend the mSEPT9 test for routine screening of colorectal cancer among Medicare beneficiaries. The scope of the NCA encompasses the use of a blood-based test for routine screening of colorectal cancer, but not among those who refuse other CRC screening modalities. The evidence from the 2020 NCCN guidelines do not support the mSEPT9 test for routine screening of colorectal cancer and does not provide benefit to Medicare beneficiaries in terms of health outcomes.
The exclusion of the blood-based SEPT9 DNA test is consistent across USPSTF (USPSTF, 2016), United States Multi-Society Task Force (Rex, 2017), ACS (Wolf, 2018), and NCCN (NCCN, 2019; NCCN, 2020) who do not recommend using Epi proColon® for routine screening of patients for colorectal cancer. The evidence/recommendations from the guidelines do not support that using the blood-based Epi proColon® test for routine screening among Medicare beneficiaries is appropriate for prevention or early detection of colorectal cancer.
Commercial Market
We assessed the commercial market for coverage of blood-based biomarker CRC screening tests. As of July 9, 2020, none of the commercial payors that we searched cover the Septin 9 test. Humana states on their medical coverage policy website for CRC screening tests, with effective date February 23, 2017, that Humana members are not eligible for Septin 9 (SEPT9) DNA methylation assay (e.g., ColoVantage, Epi proColon®) (Humana, 2017). Aetna explicitly states that they non cover the Septin 9 (Epi proColon® and ColoVantage) test. Other private payors that we have looked at do not make a statement on the Septin 9 screening test in their medical coverage policy. In our ongoing search of CRC screening tests to date, none of the commercial payors cover the Septin 9 test.
Parameters of Test Criteria
To reduce the burden on providers and to streamline implementation of the NCD, we are clarifying the parameters of the test criteria for the analytic comparison. It will be necessary to demonstrate at least equivalent test performance of a new blood-based CRC screening test. We establish the specific threshold relative to FIT since it is the most widely available screening test and has been shown to prevent CRC and improve health outcomes for patients with early stage CRC. We recognize the importance of test performance and note that there may be harms associated with utilizing a screening test with lower performance. As noted in the background, there has been a steady decline in CRC mortality due in large part to cancer prevention (removal of large or advanced adenomas before large adenomas progress to cancer) and detection of cancer at an early stage where treatments are most effective in improving survival. In a scenario where a test does not detect large adenomas or early cancer as well as currently covered tests, there may be detriments to patients since the opportunity for cancer prevention may have been missed or cancer treatments may be initiated at a later stage when health outcomes may be reduced.
Regarding FOBT, NCCN reported that “[a] Dutch randomized study… demonstrated higher detection rates of advanced neoplasia by FIT (2.4%) than guaiac FOBT (1.1%), although both were less sensitive for advanced neoplasia than flexible sigmoidoscopy (8.0%).111 In addition, as seen in other trials, FIT had a significantly higher participation rate than guaiac FOBT in this trial. Following extensive literature analysis, an expert panel in Ontario concluded that FIT is superior to guaiac FOBT in both participation rates and in detection of advanced adenomas and CRC.120” (NCCN, 2020). Comparing test performance characteristics, “there are now empirical data to suggest that FIT has higher sensitivity and specificity for CRC than HSgFOBT [high sensitivity guaiac FOBT].34” (Knudsen, 2016). The USPSTF (USPSTF, 2016) concluded that FIT has “improved accuracy compared with gFOBT.” While the evidence for FOBT/gFOBT contributes to our understanding of CRC screening tests, the evidence strongly suggests that FIT is superior to FOBT/gFOBT. Thus, the parameters for the test criteria will incorporate a comparison to FIT, but not to FOBT/gFOBT.
For estimates of test performance characteristics as a comparator to FIT, “[f]ecal immunochemical tests can be grouped according to whether they are qualitative (fixed cutoff) or quantitative (adjustable cutoff) assays; overall, test performance among this class of stool-based tests varies widely” (USPSTF, 2016). However, in the most recently published guidelines to date for colorectal cancer screening, the authors of the April, 2020 NCCN guidelines cited “[a] meta-analysis of studies that evaluated the diagnostic accuracy of FIT for CRC in average-risk patients [that] found the sensitivity to be 79% (95% CI, 0.69-0.86) and the specificity to be 94% (95% CI, 0.92-0.95).120” (NCCN, 2020). Evidence from collective data suggests that estimates for specificity and sensitivity of FIT can serve as a threshold in order to establish that a new blood-based screening test is substantially more effective than FIT and, thus, more likely to benefit asymptomatic Medicare beneficiaries when screened for colorectal cancer. The test performance characteristics of a new screening test must be as good as or better than those of FIT. For indirect evidence to support an improvement in accuracy of a new blood-based screening test for CRC in average-risk asymptomatic Medicare beneficiaries, sensitivity must be greater than or equal to 79% and specificity must be greater than or equal to 94% in the detection of colorectal cancer.
The conclusions of the Lee (2014) study focused on colorectal cancer. In the April, 2020 NCCN guidelines, the results of the Lee (2014) meta analysis (citation 120 as noted in the above paragraph) found that when using FIT the pooled sensitivity for colorectal cancer was 0.79 (95% CI, 0.69 to 0.86) and the pooled specificity was 0.94 (95% CI, 0.92 to 0.95). The authors reported that “given that only a subset of studies reported data on adenomatous polyps and that there is variability in definitions of polyps, [they] limited the scope of this analysis to test performance characteristics for detecting CRC; [they] excluded studies reporting test performance estimates for detection of adenomas only” (Lee, 2014). The authors also reported that “because of the complexity of accounting and adjusting for various definitions of advanced adenoma, the current study does not report on the performance of FIT for advanced adenoma” (Lee, 2014). The authors did not have estimates of sensitivity and specificity of FIT for detecting adenomas or early stage colorectal cancer (stage I or II) in the meta-analysis.
Below is a table of point sensitivities and specificities of stool-based CRC screening tests found in the decision memo on Screening for Colorectal Cancer - Stool DNA Testing (CAG-00440N) and found in the evidence base for blood-based CRC screening tests. The Imperiale (2014) study was also cited in the decision memo on Screening for Colorectal Cancer - Stool DNA Testing (CAG-00440N). The Lee (2014) meta analysis is cited in the this DM on blood-based CRC screening tests.
Table 4. Sensitivities and Specificities of stool-based CRC screening tests |
|
Sensitivity (%) |
Specificity (%) |
|
Colorectal cancer |
Negative colonoscopy |
Imperiale, 2014 |
|
|
Cologuard® |
92.3 |
89.8 |
FIT |
73.8 |
96.4 |
Lee, 2014 |
|
|
FIT |
79.0 |
94.0 |
As seen above, the Imperiale (2014) study shows the Cologuard® test to have a point sensitivity of 92.3% and a point specificity of 89.8%. For FIT, the sensitivities are somewhat similar, 73.8% from the Imperiale (2014) study and 79% from the Lee (2014) meta analysis. The specificities for FIT are also somewhat similar, 96.4% from the Imperiale (2014) study and 94% from the Lee (2014) meta analysis.
To foster innovation, we decided to select from across the range of estimates the lowest point threshold level for sensitivity and specificity. We selected the point sensitivity for FIT of 74% and the point specificity for Cologuard® of 90%. For the new blood-based CRC screening test, both sensitivity must be greater than or equal to 74% and specificity must be greater than or equal to 90%.
Strategy for CRC Screening Testing: Test Criteria Rather Than A Specific Test
We are issuing a Colorectal Cancer Screening (CRC) NCD that expands coverage to any blood-based biomarker colorectal cancer screening test that meets certain criteria. While Epi proColon®, one example of a blood-based CRC biomarker screening test, does not meet criteria at this time, we determined that future tests, iterations of tests, or current tests can be covered when certain patient and test criteria are met without having to reconsider the NCD. Over the last several years, blood-based biomarker tests have emerged as another potential option for the detection of colorectal cancer. Though the Epi proColon® test is currently the only FDA-approved blood-based biomarker test for colorectal cancer screening, there are other tests in development. Based on past national coverage determinations, we believe there is an established framework and examples for coverage of similar non-invasive colorectal cancer screening tests. We determined an NCD outlining the same criteria for coverage of any future or current FDA approved/cleared blood-based colorectal cancer screening tests even though there is currently no approved blood-based biomarker CRC screening test that meet the criteria. We used the same criteria when we approved the stool DNA screening test (CMS Cologuard®, 2014). The patient criteria is similar to current coverage of CRC and the same as the last CRC NCD (stool DNA). Based on the benefit and harms profiles and need for follow-up of positive tests with diagnostic and therapeutic colonoscopy, we believe non-invasive blood-based screening tests as identical to other covered non-invasive screening tests and should be considered using the same methodology. We are issuing a national coverage determination (NCD) that expands the scope of the colorectal cancer screening benefit to include coverage of any blood-based biomarker tests that meet certain patient and test criteria. Further, based on the published evidence, a non-invasive colorectal cancer screening test that meet criteria would have evidence that using the screening test would improve health outcomes for Medicare patients. Therefore, we determined criteria that is consistent with other non-invasive Medicare covered colorectal cancer screening tests.
In two past NCDs on screening fecal immunochemical tests (FIT) and stool DNA tests (Cologuard®), we determined test performance criteria that would improve health outcomes (early diagnosis, reduced mortality). Early detection of colorectal cancer provides a higher success rate for curing the cancer. While CMS does not currently have an NCD specific to screening for colorectal cancer using blood-based biomarker tests, at this point in time, Medicare covers a broad range of colorectal cancer screening tests including Cologuard® Multitarget stool DNA (sDNA) test once every 3 years which was added through a national coverage determination in 2014 under FDA-CMS Parallel Review. Screening fecal occult blood test (FOBT) every year including fecal immunochemical test (FIT) was added through a national coverage determination in 2003.
| Table 5. Point Sensitivities and Specificities of Non-invasive CRC screening tests (compared to colonoscopy) |
|
Sensitivity (%) |
Specificity (%) |
FIT |
74 |
96 |
Stool DNA test |
92 |
90 |
Epi proColon® test |
72 |
81 |
Blood-based biomarker
(use lower number from among covered tests, Table 4) |
74 |
90
|
The test performance characteristics (point sensitivity and point specificity) of the currently recommended non-invasive colorectal cancer screening tests, such as FIT and the stool DNA test, are above the blood-based biomarker test thresholds for sensitivity (74%) and specificity (90%) (Table 5).
We provide these test performance characteristics because the currently recommended, including the USPSTF, non-invasive stool-based colorectal cancer screening tests, such as FIT and the stool DNA test which are both currently covered by Medicare, have shown benefits at similar sensitivity (74%) and specificity (90%) levels, and some point estimates are above the blood-based biomarker test thresholds (Table 5).
Since Medicare covers a number of non-invasive CRC screening tests, we believe future tests should be at least as good to maintain and, ideally, to continue the reduction in CRC mortality seen over the past 20 years. This success in reducing mortality is due largely to high participation in screening with currently covered tests in the Medicare population, which leads to early detection and early treatment. When the cancer is caught early, it is curable. Since the late 1990s, Medicare has been successful in promoting early screening for colorectal cancer, covering a broad range of colorectal screening tests, both non-invasive and invasive tests. As reported in a study earlier this year among adults aged 65 – 75 years, which is within the Medicare beneficiary age range, 79 percent are up to date with currently covered Medicare tests (Joseph et al., 2020), such as stool DNA (sDNA) test, FIT, fecal occult blood test (FOBT), flexible sigmoidoscopy, and colonoscopy.
We will non-cover the Epi proColon® screening test that is FDA approved for a narrow indication for patients who have been offered and declined available CRC screening tests that are recommended by appropriate clinical guidelines, such as colonoscopy and stool-based fecal immunochemical tests (FIT). As with other laboratory tests, the FDA evaluates whether the test can detect the biomarker (clinical validity), but not necessarily whether using the screening test improves cancer survival in the general Medicare population (clinical utility). There was considerable debate before the FDA approved an uncharacteristically narrow label for the test. The FDA held an Advisory Panel meeting on Epi proColon® in March 2014. At the meeting, the staff presented that the test did not meet all of its accuracy goals when compared to testing against the older, stool-based test that is part of the paradigm of CRC screening. The advisory panel voted 5-4, with one abstention resulting in a narrow endorsement while also voting 6-5 that the test was not as effective as the comparator. Two years later, FDA approved a narrow indication in April 2016. The test received FDA approval in 2016 for average-risk patients who choose not to undergo guideline-recommended screening methods such as colonoscopy and stool-based fecal immunochemical tests (FIT).
The Epi proColon® test has a narrow indication for patients who have been offered and declined available CRC screening tests that are recommended by appropriate clinical guidelines. Patients with a positive Epi proColon® test result are referred for diagnostic colonoscopy. Yet even given this narrow indication, there is unclear evidence if a patient who has refused all other tests (patient needs to be willing to undergo screening and then diagnostic testing) or believes they cannot undergo a fecal based test that they will agree to the colonoscopy since they refused screening to begin with. The question of whether they can undergo colonoscopy (diagnostic and often therapeutic) still remains with non-invasive tests whether a stool-based test or a blood-based test. Patients who get tests that are not as good as other non-invasive stool-based screening tests may have early cancers that are missed, and may receive more false positives and then undergo more tests unnecessarily. Thus, it is difficult to
identify an appropriate population for the Epi proColon® test based on the available evidence. We could not clinically identify any patients that could not do a fecal based test, even nursing home patients. None of the societal clinical guidelines, including the USPSTF, recommend blood-based tests for routine screening of colorectal cancer or identify a vulnerable population, such as nursing home patients, that should receive a blood-based test instead of currently recommended non-invasive CRC screening tests, such as FIT or stool DNA test. No commercial payer covers any available blood-based biomarker screening test.
In this NCD, we reviewed all data, including studies sent to CMS by the requestor, Epigenomics. The studies showed that the Epi proColon® test had lower test performance for detecting colorectal cancer than other non-invasive screening tests such as the fecal immunochemical (FIT) test and stool DNA test, when used as part of routine screening for colorectal cancer.
We believe we have evaluated this test objectively, based on the previously established evidence framework for non-invasive CRC screening tests, and have applied the same criteria in determining test appropriateness for the Medicare population. This determination is consistent with the USPSTF and other professional organizations that develop clinical guidelines. No professional society organization, including the American Cancer Society (ACS) or the U.S. Multi-Society Task Force on Colorectal Cancer (including the American College of Gastroenterology), recommends any available blood-based biomarker screening test for routine screening of CRC. The USPSTF does not include this test in their recommendation for routine CRC screening. No commercial insurer covers this screening test even though it received a narrow FDA indication four years ago.
If a subsequent enhanced version of the Epi proColon® test with, for example, additional biomarkers demonstrating point specificity greater than or equal to 90% compared to colonoscopy, then that enhanced version would be an appropriate screening test for the Medicare population.
With this NCD, we are providing a pathway for Medicare coverage to support innovation and to accelerate access to emerging blood-based biomarker screening tests as soon as patient and test criteria are met. This Colorectal Cancer Screening (CRC) NCD expands the scope of the colorectal cancer screening benefit to include blood-based biomarker tests that meet certain criteria. The patient and test criteria provides a pathway for emerging tests to potentially have Medicare coverage on the same day as FDA approval. We believe the coverage pathway for future blood-based biomarker screening tests reduces burden to stakeholders of having to reconsider the NCD, and provides clear criteria to ensure stakeholders know the coverage criteria and rapid future access to blood-based screening tests for patients.
Harms of Lower Performance Screening for CRC Testing
Patients who get tests, even if the test is more convenient than other tests, that are not as good as other non-invasive stool-based screening tests may have early cancers that are missed, may receive more false positive results and then, may undergo more tests unnecessarily. Using a test,with a lower sensitivity threshold (72%) and a lower specificity threshold (81%), such as the Epi proColon®, will very likely lead to missing more cases of colorectal cancer and to more unnecessary colonoscopies. From the perspective of test performance thresholds, a worse performing test will cause more harm by missing more cases of colorectal cancer and allowing the cancer to progress, and will lead to more avoidable negative colonoscopies that might result in more unnecessary harm to the patient.
Using a test, such as the Epi proColon® test with a lower sensitivity threshold (72%), below the sensitivity threshold (74%), will lead to missing more cases of colorectal cancer (more false negative results, 26%). In addition, Epi proColon® is better at detecting late stage colorectal cancer because more of the biomarker (hypermethylated Sept9 gene) has accumulated in the blood in late stage cancer; hence, missing early stage cancer. Thus, the test is more likely to catch cancer in the later stages, potentially lowering the success rate for curing cancer. Further, this test does not prevent cancer as well as the stool DNA test, since this test does not prevent cancer by detecting large polyps that can lead to cancer; thus, missing the opportunity to remove these pre-cancerous polyps during therapeutic colonoscopy.
Using a test such as Epi proColon® with a lower specificity threshold (81%), below the specificity threshold (90%), will lead to telling patients that they have cancer when they truly do not have cancer (more false positive findings at 19%), which leads to more unnecessary negative colonoscopies.
For example in 100 patients with colorectal cancer (Table 6 below), Epi proColon® will have 20 more false negative results than the stool DNA test (20 patients with cancer would be missed, 28 – 8 = 20, also Table 11). It would also have 15 more false positive results than FIT (15 more patients would be sent for unnecessary colonoscopy that are negative, 19 – 4 = 15, Table 10).
Table 6. Example:100 patients with CRC |
False Negative – Miss CRC and Do Not Get Necessary Colonoscopy |
False Positive – Send for Unnecessary Colonoscopy |
Epi proColon® |
28 |
19 |
FIT |
26 |
4 |
Stool DNA |
8 |
10 |
To assess the harms of several CRC screening tests, we generated the data in Table 6 from a factitious patient population comprised of 100 colorectal cancer patients and 100 patients truly negative for colorectal cancer by colonoscopy, the gold standard paradigm, who were screened with Epi proColon®, FIT and a stool DNA test. Table 6 collapses the false negative findings (the test negative results that are actually positive for colorectal cancer in the lower left cell in Tables 7, 8, and 9) and the false positive findings (the test positive results that are truly negative for colorectal cancer in the upper right cell of the three tables) from Tables 7, 8, and 9.
The results of the patient screening using the known and validated point sensitivities and specificities of the three CRC screening tests are shown in Tables 7, 8, and 9 below.
Table 7. Epi proColon®: 72% sensitivity and 81% specificity |
Colorectal Cancer positive |
Colorectal Cancer negative |
Total count of patients |
Epi proColon test positive |
72 |
19 |
91 |
Epi proColon test negative |
28 |
81 |
109 |
Total patient count |
100 |
100 |
200 |
Table 8. FIT: 74% sensitivity and 96% specificity |
Colorectal Cancer positive |
Colorectal Cancer negative |
Total count of patients |
FIT test positive |
74 |
4 |
78 |
FIT test negative |
26 |
96 |
122 |
Total patient count |
100 |
100 |
200 |
Table 9. Stool DNA test: 92% sensitivity and 90% specificity |
Colorectal Cancer positive |
Colorectal Cancer negative |
Total count of patients |
Stool DNA test positive |
92 |
10 |
102 |
Stool DNA test negative |
8 |
90 |
98 |
Total patient count |
100 |
100 |
200 |
In this example, if 100 patients test negative with colorectal cancer, Epi proColon® will diagnose 19 as incorrectly positive for colorectal cancer (Table 7). These 19 will receive additional testing for colorectal cancer, which will be truly negative for colorectal cancer resulting in an unnecessary colonoscopy. The stool DNA test will find 90 patients truly negative for colorectal cancer and misidentify 10 patients as positive for colorectal cancer when in fact they do not (Table 9). Lastly, the FIT test will find 96 patients truly negative for colorectal cancer and only 4 patients incorrectly positive for colorectal cancer (Table 8). Thus, Epi proColon® will incorrectly find 9 more as positive for colorectal cancer as compared to the stool DNA test (Table 11) and 15 more patients incorrectly positive than FIT test (Table 10).
The excess false negative and false positive results are compared across the three screening tests in Tables 10 and 11 using the findings from Tables 7, 8, and 9.
Table 10. Epi proColon® compared to FIT |
Epi proColon® minus FIT (counts) |
|
| Excess false negatives (FN) |
28 – 26 = 2 |
Epi proColon® misses 2 more CRC cases beyond FIT |
Excess false positives (FP) |
19 – 4 = 15 |
Epi proColon® tells 15 more patients that they have cancer when they do not, leading to 15 more unnecessary negative colonoscopies, beyond FIT |
| Table 11. Epi proColon® compared to stool DNA test |
Epi proColon® minus stool DNA test (counts) |
|
Excess false negatives (FN) |
28 – 8 = 20 |
Epi proColon® misses 20 more CRC cases beyond the stool DNA test |
| Excess false positives (FP) |
19 – 10 = 9 |
Epi proColon® tells 9 more patients that they have cancer when they do not, leading to 9 more unnecessary negative colonoscopies, beyond the stool DNA test |
Increased adherence because of more convenience to a lower performance CRC screening test, such as Epi proColon®, can lead to missing more cases of colorectal cancer and more unnecessary colonoscopies when compared to the currently recommended (by societies and USPSTF) and FDA approved non-invasive screening tests, such as FIT and the stool DNA test, for routine screening of colorectal cancer. The Epi proColon® test does not prevent colorectal cancer as well as FIT or stool DNA test.
Implementation of Threshold Test Performance Criteria
We recognize the potential advantages of having a wide range of options in CRC screening to optimize screening and health outcomes. As we have noted in prior CRC screening NCDs, we consider direct and indirect evidence on health outcomes. Test performance in detecting large, advanced adenomas and early stage cancer are important to achieving improved outcomes. Medicare covers a number of recommended screening tests and a new test should be as good as, or ideally better than, the current screening test to continue the progress achieved in colorectal cancer survival over the past 20 years. We are proposing a pathway for future Medicare coverage if specific criteria are met to increase appropriate access without having to reconsider the NCD. To determine the decision threshold for coverage of a new CRC screening test, we suggest utilizing data from the FDA label to compare test performance characteristics. Because the FDA label includes the results from the pivotal study, the sensitivity and specificity of the new screening test can be compared to the threshold test criteria for sensitivity (≥ 74%) and specificity (≥ 90%). The analysis of sensitivity and specificity will be valid as long as the pivotal study incorporates colonoscopy as the gold standard comparator to the new CRC screening test. If the pivotal study does not estimate the sensitivity and specificity of the new blood-based CRC screening test, then the test performance characteristics may come from another published comparative clinical study that has colonoscopy as the gold standard comparator. The results of the analysis for the new blood-based CRC screening test must be generalizable to the Medicare population.
For Epi proColon® test, if a subsequent enhanced version with, for example, additional biomarkers demonstrated point specificity greater than or equal to 90% compared to colonoscopy and was included in a professional organization recommendation, then that enhanced and recommended version would be appropriate screening test for the Medicare population,
Implementation of Statutory Requirements
Medicare coverage of CRC screening tests is contingent on meeting statutory requirements. We provided criteria in the NCD language to ensure these requirements are met and to facilitate coverage of these tests in the future. We believe that along with FDA approval that inclusion as a colorectal cancer screening option in at least one professional society guideline or consensus statement or USPSTF recommendation would provide strong support in meeting the requirement to expand coverage in consultation with appropriate organizations.
Frequency of testing
We did not find evidence on the frequency of CRC screening using a blood-based biomarker test. The frequency of screening with blood-based CRC screening tests has not been definitively established, since cross-sectional observational studies usually provide evidence at one point in time (one screening in this case). Thus, these studies do not provide direct evidence on how often any particular test should be performed. The authors of the 2019 and 2020 NCCN guidelines report that “the interval for repeating [SEPT9 DNA] testing is unknown” (NCCN, 2019; NCCN, 2020). The authors of the US Multisociety Task Force guidelines state that “the best frequency for performing the [Septin9] test is uncertain” (Rex, 2017). We looked to the FDA approved stool DNA testing decision memo on Cologuard (CMS, 2014) for an established analytic framework to determine frequency of screening for a blood-based CRC screening test. The 2019 NCCN guidelines report that for a combined multitarget stool DNA and occult blood test (mt-sDNA) which is the Cologuard (Exact Sciences) test, “a rescreening interval of every 3 years has been suggested and is approved by the FDA” (NCCN, 2019). With the natural history of most colorectal neoplasia and improved test performance of the new blood-based screening test, screening every three years appears to be a reasonable initial frequency to detect clinically meaningful changes. Since the methodology and analytic approach for CRC screening tests have been used consistently for past considerations, we determined a frequency of every three years to match the frequency of coverage for FDA approved stool DNA testing based on a similar rationale of benefits and harms.
Assessment and Analysis of Published Articles Submitted by Public Commenters
We received 47 references with the public comments. All were reviewed but only eight were included in the analysis. Thirty-nine were not included because they related to other non-invasive CRC tests such as FIT, invasive tests such as colonoscopy, mechanisms of action such as metastasis, policy statements on cancer treatment or cancer mortality, cancer statistics, and guideline topics beyond the scope of the NCD such as a reporting checklist, or trends in age of colorectal cancer diagnosis. Appendix E contains a list of those references reviewed but not included in the analysis.
Modeling Studies
In the D’Andrea (2020) study, the authors “developed and validated a microsimulation model to simulate colorectal cancer incidence and mortality based on observed data.” They used the microsimulation model to assess the effectiveness of ten screening strategies in terms of CRC incidence and mortality, incremental life years gained (LYG), number of colonoscopies, and adverse events for men and women 50 years or older over their lifetime. They evaluated ”ten different screening strategies (8 screening modalities): (a) no screening (NS); (b) flexible sigmoidoscopy every 5 years (FS); (c) colonoscopy every ten years (COL); (d) annual fecal immunochemical testing (FIT); (e) annual high-sensitivity guaiac-based fecal occult blood testing (HS-gFOBT); (f) multitarget stool DNA testing every 3 years (FIT-DNA); (g) computed tomographic colonography every 5 years (CTC); and (h) the methylated SEPT9 DNA blood test (SEPT9) with 1, 2, and 3 year intervals.”
They “assessed outcomes under 100% adherence rates and reported adherence rates.” “To model the reported adherence scenario, [they] derived data on the one-time adherence rates for each strategy from the published literature….For the SEPT9 blood test, we assumed an 85% one-time adherence rate in the base case analysis and varied it between 25% and 95% in the sensitivity analyses, as we did for all other strategies. Our assumptions about adherence to SEPT9 were based on results of a randomized trial in the US in which 99.5% of subjects overdue for screening chose to take the blood test, [Liles, 2017]6 and a study in Germany in which 83% of patients refusing colonoscopy selected the SEPT9 blood test. [Adler, 2014].”
They “built a microsimulation model [also called the PREDICT model] using Arena Version 15.00 (Rockwell Automation Technologies, Inc.) that simulates the natural history of CRC, to compare clinical benefits, harms, and burden of testing for alternative strategies for CRC screening. [They] created a hypothetical cohort of individuals age 50 years or older, which emulated the distribution of baseline characteristics for subjects in landmark clinical studies. [They] then created identical cohorts and assigned them to different screening strategies to compare intervention related differences in outcomes. For each strategy, [they] simulated 1000 trials, for a cohort of 10,000 individuals (i.e., 10,000,000 simulations per strategy).”
For the results, “assuming 100% adherence, FIT-DNA every three years, FIT, HS-gFOBT, and SEPT9 annually averted 42 to 45 cases and 25 to 26 deaths per 1000 individuals screened; COL averted 46 CRC cases and 26 CRC deaths and CTC averted 39 CRC cases and 23 CRC deaths per 1000 individuals screened; and FS averted 32 CRC cases and 19 CRC deaths per 1000 individuals screened. Estimated LYG were similar across FIT-DNA, FIT, HS-gFOBT, SEPT9, CTC, and COL strategies.”
Assuming published adherence rates, “SEPT9 every year averted 37 CRC cases and 23 CRC deaths per 1000 individuals screened; COL averted 34 CRC cases and 20 CRC deaths per 1000 individuals screened; FS, FIT-DNA, FIT, CTC and HS-gFOBT averted approximately 16 to 25 CRC cases and 11 to 16 CRC deaths per 1000 individuals screened…. LYG reflected the effectiveness of each strategy in reducing CRC cases and deaths…. The total number of colonoscopies was highest in the COL strategy (1897), followed by SEPT9 every year (1708), FIT-DNA (568), FIT (379), HS-gFOBT (377), CTC (305), and FS (199). The number of adverse events (perforation or major bleeding) was highest in the COL strategy (3.7 per 1000 individuals screened), followed by SEPT9 every year (3.4 per 1000 screened), CTC (1.5), FIT-DNA (1.1), HS-gFOBT (0.8), and FIT (0.8), and FS (0.6).”
The authors found that “In the ideal condition of full adherence, screening with stool-based tests (i.e., FIT-DNA, FIT, HS-gFOBT), CT colonography, or annual SEPT9 would produce comparable benefits to screening with colonoscopy every ten years. However, when we modeled reported adherence rates, the results changed substantially: colonoscopy appears superior in reducing cancer incidence and mortality over all other USPSTF recommended CRC screening methods while annual SEPT9 is predicted to be an effective non-invasive option for patients unwilling or unable to use the other modalities. The findings suggested that adherence rates higher than 65%-70% would be required for any stool or blood-based screening modality to achieve the benefits of colonoscopy.” More specifically, the authors reported that “at 100% adherence, the stool-based tests and SEPT9 showed a clinical performance similar to that of colonoscopy. Although these tests have a substantial lower one-time sensitivity than colonoscopy, the frequent testing and shorter test interval increases the overall probability of cancer detection over time…. In addition, the results of the stool- and blood-based tests might be slightly overestimated because we did not model a decline in sensitivity over time.” For the SEPT9 DNA test, “However, additional data on compliance are needed to establish the actual adherence rates in a real-world setting, and across alternative screening options.” (D’Andrea, 2020).
One limitation reported by the authors was that “in the absence of data on the programmatic performance of screening modalities, we assumed that the sensitivity and specificity of all tests remained constant. This limitation can affect our relative findings, potentially overestimating sensitivity, but also overestimating the false referral rate. It would have a smaller impact on tests with longer intervals, such as colonoscopy and CTC, compared to tests with shorter intervals.” Another reported limitation is that “in the evaluation of reported adherence rates, we assumed that individuals remained adherent to their initial screening modality over time. In clinical practice, patient adherence may vary from year to year, and these gaps in continuous screening are more likely for modalities with shorter time intervals. Thus, the clinical benefits gained using strategies such as stool-based tests and the SEPT9 blood test might be slightly overestimated in our model.” A further limitation is that “data on studies that have reported on adherence rates are limited and can vary across different populations, healthcare systems, and geographies.”
The authors concluded that “Adherence rates higher than 65%-70% would be required for any stool or blood-based screening modality to match the benefits of colonoscopy.”
In the Peterse (2020) cost effectiveness analysis study, “the Microsimulation Screening Analysis-Colon (MISCAN-Colon) model was used to evaluate the [comparative] cost-effectiveness of screening with capsule endoscopy every 5 or 10 years, computed tomographic colonography every 5 years, the multi-target stool DNA (mtSDNA) test every 1 or 3 years, and the methylated SEPT9 DNA plasma assay (mSEPT9) every 1 or 2 years. The authors also compared these strategies with annual FIT screening and colonoscopy screening every 10 years.”
For the Methods, the MISCAN-Colon model is part of the US National Cancer Institute’s Cancer Intervention and Surveillance Modeling Network (CISNET). “In brief, the model generates, with random variation, a large population similar to the US population in terms of life expectancy and CRC risk. As each simulated person ages, 1 or more adenomas may develop, which can progress in size and can develop into preclinical cancer (stages I-IV). During each stage, CRC may be diagnosed because of symptoms. Screening can alter some simulated life histories, because CRC can be prevented or diagnosed at an earlier stage. Screening may also result in complications, overdiagnosis, and overtreatment, which are also taken into account by the model.” The authors “simulated screening from age 50 years through 75 years in an average-risk population, with perfect adherence to screening, diagnostic follow-up, and surveillance recommendations.” “To compare the different screening strategies, an incremental cost-effectiveness analysis was performed, ranking strategies based on costs.” The authors “evaluated a scenario in which 12% of the advanced adenomas and 18% of CRCs were systematically missed by the mSEPT9 due to no methylation of the SEPT9 gene promoter.”
For the Results, for individuals who are not willing to undergo FIT or colonoscopy screening (i.e., those for whom FIT and colonoscopy are not considered acceptable alternatives), “Among the alternative tests, computed tomographic colonography every 5 years, annual mSEPT9, and annual multi-target stool DNA screening had incremental cost-effectiveness ratios of $1092, $63253, and $214974 per quality-adjusted life-years gained (QALYG), respectively.” “Under the assumption of perfect adherence, annual mSEPT9 screening resulted in more QALYG, CRC cases averted, and CRC deaths averted than annual FIT screening but led to a high rate of colonoscopy referral (51% after 3 years, 69% after 5 years)….However, the test burden in terms of number of diagnostic colonoscopies was 63% higher, and the total costs were 26% higher compared with annual screening with FIT.”
The authors concluded that “This study suggests that for individuals not willing to participate in FIT or colonoscopy screening, mSEPT9 is the test of choice if the high colonoscopy referral rate is acceptable to them.” The authors reported that “The uncertainty of our conclusion is reflected in our probabilistic sensitivity analyses in which the mSEPT9 was the cost effective strategy in 54% of our analyses. Test accuracy of the mSEPT9 is not as well established as for some of the other tests evaluated in this study.”Further, “Among the tests evaluated in this analysis, the mSEPT9 has the lowest sensitivity for both adenomas and CRC. Therefore, an important driver of its cost-effectiveness compared with CTC, PillCam, and mtSDNA is the substantially lower cost of the test.”
“Due to the relatively low specificity of the mSEPT9 (79%) compared with the other tests, a high number of individuals are referred to a diagnostic followup colonoscopy regardless of disease status (51% after 3 years and 69% after 5 years with annual repetition of the test). Consequently, 21% of simulated individuals with a nonadvanced adenoma received a colonoscopy when screened with mSEPT9 in
contrast with 7.6% when screened with FIT…. Although nonadvanced adenomas generally confer low risk, they are more common than advanced adenomas and some may have aggressive biology. The detection of nonadvanced adenomas in these colonoscopies contributed to the slightly higher QALYG, CRC cases averted, and CRC deaths averted for mSEPT9 screening vs FIT screening despite its lower test sensitivity for advanced adenomas and cancers.”
A limitation reported by the authors is that they “assumed perfect adherence to screening, diagnostic follow-up, and surveillance in our base case analysis. This implies that the model predicted the maximum achievable benefit for all screening tests. Unfortunately, there are limited data on test-specific adherence to every step in the screening process (getting screening, diagnostic follow-up, treatment and/or surveillance) over multiple rounds of screening (e.g., from ages 50 years to 75 years), making it impossible to inform our analyses with empirical evidence.”
The authors concluded that “a well-established microsimulation model demonstrates that for people who are unwilling to be screened with FIT or colonoscopy, annual screening with the mSEPT9 is the test of choice given its cost-effectiveness profile compared with CTC, PillCam, and mtSDNA…. However, the number of colonoscopies required for the mSEPT9 is 63% higher, and the total costs are 26% higher compared with annual FIT screening. Therefore, physicians should first offer individuals to participate in CRC screening using FIT or colonoscopy.”
There are challenges when considering the usefulness and applicability of modeling studies. For instance, it is unclear if modeling results should be considered on par with empiric evidence generated from studies on humans. How the USPSTF uses modeling studies should also be taken into consideration.
Modeling and Empiric Evidence
In Owen’s 2016 study on the use of decision models by the USPSTF, “The USPSTF considers using decision modeling only for preventive services for which there is either direct evidence of benefit in clinical trials, at least for some populations, or indirect evidence of benefit established through the linkages in the analytic framework (Figure 1) based on the systematic evidence review [reference]” (Owens, 2016). The authors of the Owens (2016) study discussed how “Decision modeling is useful when clinical questions remain about how to target an empirically established clinical preventive service at the individual or program level or when complex determinations of magnitude of net benefit, overall or among important subpopulations, are required. Before deciding whether to use decision modeling, the USPSTF assesses whether the benefits and harms of the preventive service have been established empirically, assesses whether there are key issues about applicability or implementation that modeling could address, and then defines the decision problem and key questions to address through modeling” (Owens, 2016). Thus, it appears that the USPSTF first establishes the benefits and harms of a clinical preventive service, such as colorectal cancer screening, based on empiric evidence before deciding on whether to use decision modeling. Then the Owen (2016) study suggests that decision modeling is used to answer key questions on applicability or implementation of the clinical preventive service, rather than on the benefits or harms, such as cancer survival, of the preventive service. As a result, the D’Andrea (2020) microsimulation study and the Peterse (2020) cost effectiveness microsimulation study were not included in our systematic review of the evidence of blood-based colorectal cancer screening tests.
In the development of recommendations for preventive services, the USPSTF “typically requires deliberation using comprehensive systematic reviews of the best available evidence and a series of complex judgments. These include integrating evidence about benefits and harms from randomized, clinical trials and observational studies; assessing whether benefits outweigh harms and, if so, by how much and in which populations; assessing the degree of certainty the evidence provides for both benefits and harms; and determining ages and other risk factors needed to specify when to begin and stop offering the service and in which populations” (Owens, 2016). Owens et al. (2016) reported that ““Direct evidence [of benefit] comes from a clinical trial that evaluates the preventive service and assesses health outcomes of importance to patients, such as disease-specific mortality, total mortality, or quality of life.” (Owens, 2016). These findings suggest that the USPSTF relies on the empiric evidence from randomized clinical trials and observational studies on humans to establish the benefits and harms based on mortality of a preventive services and does not rely on modeling studies for such an assessment.
Further in Petitti’s (2018) article on the USPSTFs experience and perspective on using modeling to support evidence-based policy recommendations on preventive services, the authors reported that “Models can bridge empiric evidence to inform decisions and help develop guidelines[references]” (Petitti, 2018). Moreover, from the perspective of the USPSTF, “The framework developed by the USPSTF [reference] will help determine when to use modeling as a complement to systematic reviews…”(Owens, 2016). However, there is no mention of using modeling to replace empiric evidence in the systematic review to address questions about CRC screening tests.
USPSTF’s Experience with Modeling
The authors of the Petitti (2018) study reported that “The USPSTF used information from collaborative modeling in its 2008 and 2016 colorectal cancer screening recommendations, [ref.] and in its 2009 and 2016 breast cancer screening recommendations. [ref.] For both the colorectal cancer and breast cancer screening topics, modeling informed recommendations about screening interval and starting and stopping age for screening” (Petitti, 2018). However, the authors did not mention using modeling to assess the impact of a colorectal cancer screening test on cancer survival or mortality. It appears that the USPSTF does not use modeling to assess clinical utility of a colorectal cancer screening test. Instead, “Direct evidence [of benefit] comes from a clinical trial that evaluates the preventive service and assesses health outcomes of importance to patients, such as disease-specific mortality, total mortality, or quality of life” (Owens, 2016). Thus, the Owens (2016) study suggests that the USPSTF assesses mortality from empiric evidence to establish the clinical utility of a preventive service, such as a colorectal cancer screening test.
Uncertainty in Modeling
The van Ballegooijen, Rutter, et al. (2011) study demonstrates the uncertainty resulting from the variability inherent in colorectal cancer screening models, likely from the differences in assumption, that project wide differences in potential effectiveness of colorectal cancer screening. CISNET published some evaluations of the variability inherent in their modeling results in colorectal cancer screening by evaluating how the different assumptions among the models may drive outcomes by pointing out the between-model differences in projected effectiveness. In a van Ballegooijen, Rutter, et al. (2011) study of microsimulation models, the authors projected “the cost-effectiveness of colonoscopy screening for the three microsimulation models.” The authors used a measure called maximum clinical incidence reduction (MCLIR) to explain the impact of different assumptions between models resulting in wide differences in projected effectiveness, 52-91% for incidence reduction; 65-92% for mortality reduction.
The authors concluded that “There are considerable between-model differences in projected effectiveness” (van Ballegooijen, Rutter, et al., 2011). The authors reported that “By comparing the MCLIRs between models, similarities or differences in natural history, and more specifically, the models' implicitly assumed length of the preclinical disease phase, become apparent” (van Ballegooijen, Rutter, et al., 2011). The findings suggest that the variability in the modeling results are likely due to differences in assumptions about the natural history and the length of the preclinical disease phase for colorectal cancer. Differences in the magnitude and direction of the modeling results are likely to depend on the assumptions that are the inputs into the simulation models.
Modeling and Cost effectiveness Studies
In the Peterse (2020) cost effectiveness analysis study, “the Microsimulation Screening Analysis-Colon (MISCAN-Colon) model was used to evaluate the cost-effectiveness of screening with capsule endoscopy every 5 or 10 years, computed tomographic colonography every 5 years, the multi-target stool DNA (mtSDNA) test every 1 or 3 years, and the methylated SEPT9 DNA plasma assay (mSEPT9) every 1 or 2 years. The MISCAN-Colon model is one of three models that are part of the US National Cancer Institute’s Cancer Intervention and Surveillance Modeling Network (CISNET). “Questions surrounding the comparative- and cost-effectiveness of colorectal screening tests led to the development of the three colon microsimulation models” (NCI, https://resources.cisnet.cancer.gov/registry/site-summary/colorectal/. Accessed December 3, 2020.). We do not consider cost in our systematic review of the published evidence. Thus, the Peterse (2020) cost effectiveness microsimulation study was not included in our systematic review of the evidence of blood-based colorectal cancer screening tests.
Analysis of Modeling Studies
While simulation modeling can be valuable tools that contribute to our understanding of colorectal cancer screening, there are challenges, such as uncertainty and USPSTFs approach, around the usefulness and applicability of modeling studies, including the D’Andrea (2020) microsimulation study of the effect of adherence to different screening strategies, including the mSEPT9 test, on life years gained and CRC incidence and mortality, and the Peterse (2020) microsimulation cost effectiveness CISNET modeling of using the mSEPT9 plasma assay on QALYG and mortality study as cited by the sponsor. Thus, neither the D’Andrea (2020) microsimulation study nor the Peterse (2020) cost effectiveness study were included in our internal technology systematic review of the published primary evidence.
Adherence
The Liles (2017) study compared “uptake of an experimental blood test with that of a FIT for colorectal cancer screening in an office setting” (Liles, 2017). “This small two-site randomized controlled trial (ClinicalTrials.gov, ID NCT02251782) [randomly] assigned 413 average-risk adults overdue for screening in an integrated health system to one of two arms: Offer of a FIT versus offer of a blood test [Epi proColon} for colorectal cancer screening…. The trial enrolled individuals overdue for screening in spite of recent offers by mail or phone” (Liles, 2017). For enrollment, “From December 2014 to March 2015, study sites identified adults 50–75 who were overdue for screening” (Liles, 2017). The authors “randomly assigned participants to receive screening with either an investigational use only blood test (Epi proColon, Epigenomics Inc., Seattle, WA) or a FIT (OC-FIT Chek, Polymedco, Cortlandt Manor, NY). The study sponsor generated the randomization sequence centrally and distributed sealed allocation envelopes to the two sites; research staff members were blinded to allocation until enrollment… All participants who did not complete the assigned test within 4 weeks received a reminder postcard…. All participants received a $25 gift card…. Participants with a positive test result also received a phone call within one week of the result, and a referral for colonoscopy. If the participant did not have a colonoscopy scheduled 4 weeks after the referral date, we sent a reminder postcard” (Liles, 2017). The mean age was 59.2 years (standard deviation = 6.0).
For the results, “9347 participants received invitation letters. Of these, 490 enrolled, of which 413 were eligible” (Liles, 2017). Within six weeks of the offer, “99.5% (95% confidence interval: 97.3%-100%) of participants in the blood test arm and 88.1% (95% CI: 83.0% − 91.8%) of participants in the FIT arm completed the offered test, a difference of 11.4% (95% CI: 6.9% − 15.9%, p < .001). 16.5% [30 out of 182] of participants in the blood test arm and 1.7% [3 out of 179] of participants in the FIT arm had a positive test. 20 of 30 [66%] and 2 of 3 [66%] in the blood test and FIT arms, respectively, either scheduled or completed a colonoscopy within 3 months of the positive test result” (Liles, 2017). “Two of the three FIT-positive participants scheduled a colonoscopy; one completed it within 3 months, with the finding of a single hyperplastic polyp. For the 30 patients who tested positive using the blood test, 20 scheduled a colonoscopy and 17 completed it within 3 months. For the Epi proColon positives, 10 patients had some reported lesion, of which there were 3 tubular adenomas, 4 serrated polyps of colonic mucosa, 1 inflammatory polyp, and 2 hyperplastic polyps were reported.” (Liles, 2017).
The authors reported that “Some limitations of our study may limit the generalizability of our findings. Rates of screening uptake within six weeks of a screening were unexpectedly high—88.1% in the FIT group and 99.5% in the blood test group. These were notably greater than screening uptake within usual care, which was 20.2%. Also, some study procedures (e.g., compensation), focus on CRC screening in the practice environment, and awareness of participating in a study likely resulted in a higher than usual adherence for both arms [reference]. The face-to-face enrollment visit (a strict requirement for an experimental test) likely also biased the enrolled population toward those more willing to screen [reference]. Although we included participants who had not screened in spite of multiple reminders, many were willing to screen when counseled in person [reference]. Finally, the proportion of Latinos in our population ( < 6%) was lower than that in the U.S. Census (17.4%) [references]; differences in health beliefs and practices may limit applicability to this demographic. Nonetheless, randomization of participants, standardized counseling scripts, and identical reminder letters between groups allowed for a balanced comparison of screening behavior” (Liles, 2017)
Further, the authors did report that “Epi proColon had a high false positive rate (16.5%) for detecting CRC in comparison to the OC FIT Chek (1.7%); neither test detected any colorectal cancers. This is similar to the 18.5% false positive rate found for Epi proColon in a previous study (OC FIT Chek, 2.4%) [reference]. We did not explain false positive rates of the fecal and blood tests to participants prior to enrollment; we wanted to deliver succinct counseling to simulate primary care.”
The authors concluded that “In our small randomized controlled trial, completion of a blood test for colorectal cancer screening was 11.4% higher than completion of a fecal immunochemical test, among adults overdue for screening. A blood test for adults hesitant to use other CRC screening methods may be a useful option” (Liles, 2017).
We received public comments on adherence, advanced adenoma, potential unintended consequences of a high false positive rate, and sensitivity and specificity. We also made changes to the criteria for screening frequency and screening age. We also provided an update on the USPSTF’s 2020 draft recommendation on colorectal cancer screening.
Analysis of Adherence Study (Liles, 2017)
A major limitation of the Liles (2017) study is that the investigator did not explain the false positive rate, telling the patient that they are likely to have colorectal cancer when they in fact do not, which leads to an avoidable colonoscopy, another harm resulting from a false positive test result, for either the Epi proColon test or the FIT test during the enrollment process. In addition, the investigators did not explain the harms of the false negative rate, telling the patient that they do not have cancer, when they may have colorectal cancer leading to not having the appropriate follow up colonoscopy and the harm of missing the diagnosis of colorectal cancer. It is not clear from the study results what the effect of this discussion of test error rates with the participant would have on uptake of the CRC screening tests, especially in light of the goals of shared decision making. In this study, among all Epi proColon positive tests, no cases of colorectal cancer was found.
Another major limitation is that of 9347 individuals who were invited to participate, only 5.2% (n=490) enrolled in the study, meaning that most, 94.8%, of the target population did not respond. It is possible that selection bias might lead to volunteer bias, such that only those individuals who had a healthy lifestyle and were motivated to enroll in the research study participated which could result in an overestimate of adherence to screening in both study arms, with such a bias leading to an erroneous conclusion from the data.
Additionally, there was no difference in the proportion (66%) of participants with positive results who either scheduled or completed a colonoscopy within 3 months of referral, meaning that having a positive blood-based test did not increase follow up colonoscopy rates when compared to a positive FIT. Combining patients who scheduled a colonoscopy with those who completed a colonoscopy is an issue because scheduling a colonoscopy does not necessarily mean a colonoscopy was completed. Thus, there was no difference in adherence to follow up colonoscopy when comparing Epi proColon to FIT.
Other major study design limitations include that the Usual Care group was not part of the random allocation process. It is possible that the Usual Care Group was drawn from a different study population than the study population from which the FIT / blood test intervention group was drawn from. Thus, any differences in uptake compared between the two groups could be confounded by differences in demographic composition, for example, leading to misinterpretation of the results and an erroneous conclusion. This could lead to an unbalanced, and thus biased, comparison of screening behavior.
Another major limitation of the Liles (2017) study is the setting of the study might affect generalizability since the experience of a screening program within an integrated health system might be different from the experience in the general community population. Thus, the results of the Liles (2017) study might not be generalizable to the Medicare population.
It is unlikely that all Medicare beneficiaries in the general community population will have the advantage of participating in an integrated health system that provides scripted counseling about the CRC screening options that was likely a meticulous, intensive and systematic follow up discussion of CRC screening options with the patient. Thus, the study results might overestimate adherence compared to the general population living in the community.
The authors point out the small sample size as a limitation of their study. The numerator data consisted of numbers with a small magnitude. For instance, the number of positive tests was small, 3 of 179 (1.7%) for FIT and 30 of 182 (16.5%) for the blood-based test.
In addition, there was no blinding of the participants or the investigators to the intervention in this randomized study. The lack of blinding might lead to a differential response bias by the participants or interviewer bias in the face-to-face enrollment visit by the investigators outside of the standardized counseling script, leading to differences in uptake between the two arms due to the participants knowing which intervention was being administered to them, and the investigators and participants knowing the purpose of the research study. The authors reported that the “face-to-face enrollment visit (a strict requirement for an experimental test) likely also biased the enrolled population toward those more willing to screen [reference].” (Liles, 2017). Additionally, the investigators reported that lack of blinding would lead to “awareness of participating in a study likely resulted in a higher than usual adherence for both arms [reference]” (Liles, 2017). The lack of blinding could lead to an unbalanced comparison of screening behavior, leading to potentially erroneous
conclusions.
All participants received a gift card as an inducement to enroll in the study, likely biasing enrollment upwards which could affect generalizability of the findings to the general community population which has no such inducements available as a part of a CRC screening program. It is likely that incentivizing participation in the study might lead to an overestimate of the effect of the screening program due to the extra motivation to enroll in the study.
While the results are intriguing, two areas of concern for the Liles (2017) study are the generalizability of the findings to the Medicare population, due to the limitations such as bias, and whether the outcome measures, by not assessing incident cancer cases, are the most relevant outcomes to improving the health of the Medicare beneficiaries. The conflicts of interest and the biases and limitations inherent in the study design might lead to erroneous conclusions being drawn from biased data. Thus, it is difficult to assess the validity of the conclusions of the Liles (2017) adherence study, as well as the generalizability of the study uptake results to the Medicare population.
Rationale for Changes to Screening Frequency
We have adjusted the frequency interval for colorectal cancer screening with a blood-based biomarker test to once every 3 years with expedited adjustment if evidence supports such a change in the future. The rationale for this change is to maintain consistency with the past national coverage determination on a non-invasive colorectal cancer screening test based on similar evidence. The framework for the national coverage determination that approved the stool DNA screening test (CMS Cologuard®, 2014)
has evidence that supports a testing interval of once every 3 years. We removed the FDA determination of CRC screening test frequency from the decision language. Applying a similar framework to the blood-based biomarker test, the frequency of screening with a blood-based colorectal cancer screening test will be once every three (3) years.
Analysis of Sensitivity and Specificity
Our framework to specifying both the point sensitivity and point specificity was to have an evidence based approach as the foundation for the decision. The rationale was that such an evidence based approach would provide transparency to our decision making process for providing specific cutpoints for sensitivity and specificity. Such an evidence based approach is reproducible in that anyone can recreate the decision process that went into identifying the cutpoints. In order to access the most up to date evidence, we reviewed the most recent published CRC guidelines available, the NCCN 2020 practice guidelines on colorectal cancer screening (NCCN, April, 2020). The April 2020 NCCN colorectal cancer screening guideline did not have any information on potential cutpoints for sensitivity and specificity of a blood-based screening test. But the 2020 NCCN guidelines did have a meta analysis, the Lee (2014) study, that reported pooled point estimates for sensitivity and specificity for FIT, a widely available non-invasive CRC screening test. We believe the Lee (2014) study provided high quality evidence for the pooled estimates since the estimates came from collective data integrated across 18 articles that described 19 cohort studies (Lee, 2014). The mean age of the study populations ranged from 45.2 to 62.7 years (Lee, 2014). Use of the pooled estimates from across different study populations is likely to enhance generalizability of the meta analysis pooled results to the Medicare population. We wanted to maintain consistency with the evidence based framework of past screening test decisions and utilized the test performance characteristics from the previous decision on the stool DNA screening test (CMS Cologuard®, 2014), another widely available non invasive colorectal cancer screening test. Thus, we believe the evidence based framework provided the highest quality evidence to specify cutpoints for sensitivity and specificity that was available in the published literature.
We decided not to change the pre-specified point sensitivity and specificity that is in the decision memo. Given the inverse relationship between sensitivity and specificity, we could not provide an adequate rationale for altering the pre-specified cutpoints. If sensitivity was increased, then specificity would decrease for a screening test. If specificity was increased, then sensitivity would decrease. We felt that the pre-specified cutpoints allowed for a balance of the false positive rate against the false negative rate for the screening test. Thus, we believe that the pre-specified test performance characteristics would yield the most reasonable balance of the benefits and harms of the blood-based CRC screening test based on the limited evidentiary science available.
We also believe that having pre-specified test performance characteristics does not stifle innovation, and in fact promotes competition. We felt that having pre-specified cutpoints provides a targeted goal for manufacturers when they develop their blood-based screening test. We think that competitive market forces will encourage manufacturers to develop screening tests with sensitivities and specificities above the minimum standard cutpoints. Competition in the commercial market place is likely to encourage subsequent iterations of blood-based screening tests that would continue to improve upon test sensitivity and specificity.
We considered alternative language for the policy statement on point sensitivity and point specificity. We considered not specifying an actual number for the point sensitivity or specificity but then implementation of the policy would be a challenge. For example, stating that sensitivity and specificity had to be “high” is problematic in that it is not clear how to define an appropriate code for “high” sensitivity test that would allow for reimbursement of the screening test. We also considered reverting back to requiring a head-to-head comparison to FIT but we believe this would place an immense burden on the manufacturers and stifle innovation. We were unable to develop any other satisfactory alternative language that did not have its own challenges in implementation of the policy statement on blood-based colorectal cancer screening.
In the Analysis section above on Harms of Lower Performance Screening for CRC Testing that was about screening test false positive and false negative rates, the discussion had a focus on screening test error rates. The purpose of this discussion was to describe the harms of the false positive and the false negative test result from a one-time screening using Epi proColon® compared to FIT. We describe the tradeoff relationship between low sensitivity and high false negative rate, leading to a harm of incorrectly telling a patient that they do not have cancer resulting in missing more cases of colorectal cancer when using Epi proColon®. Additionally, we show the tradeoff between low specificity and a high false positive rate, leading to the harm of incorrectly telling a patient that they have cancer when they do not, resulting in more unnecessary negative colonoscopies beyond FIT. This section was not a discussion of the inverse relationship between sensitivity and specificity. We show that low test performance characteristics, i.e., sensitivity and specificity, can lead to high CRC screening test error rates, i.e., false positive and false negative test rates.
Analysis of High False positives and Unintended Consequences of High False Positive Rate by Ransohoff (2020)
In an editorial by Ransohoff (2020), he considered policy decisions about mSEPT9 that may have consequences that are unintended, unusual, and clinically significant by addressing three questions.
First, what are mSEPT9’s sensitivity and specificity, and what are implications of a high false-positive rate (20%) for a test intended to be used by persons “unwilling” to have a colonoscopy?
The author wrote that “The FDA was concerned that the 20% false-positive rate could cause many persons without CRC to be recommended for colonoscopy—a problem for a test intended for persons unwilling to have colonoscopy or FIT. Another concern was that an advised colonoscopy might not be accepted after a positive mSEPT9. The FDA asked the sponsor to assess adherence among persons unwilling” to have FIT or colonoscopy, that is, among intended screenees. The Liles study (7) assessed 182 compensated participants who completed the mSEPT9 test. Among 30 participants with a positive mSEPT9, 23 had a colonoscopy or agreed to one by the end of the study (7). Clear detail is not provided, however, about how participants’ “unwillingness” to have FIT or colonoscopy was assessed. A “scripted telephone interview” was conducted “to confirm selected inclusion criteria,” but the wording of the script was not reported (7). Further, Liles (7) notes, “We did not explain false-positive rates of the fecal and blood tests to participants before enrollment; we wanted to deliver succinct counseling to simulate primary care.” It is hard, then, to understand the magnitude of the problem of adherence without knowing “how unwilling” participants were to have colonoscopy at enrollment” (Ransohoff, 2020).
“When the FDA approves a diagnostic test, it may issue a Summary of Safety and Effectiveness Data (SSED), where some of these issues might be addressed (8). The SSED is written by the sponsor and then approved by the FDA as part of the product’s labeling. The 2016 SSED devotes most of its 41 pages to technical issues, including limits of detection, specimen stability, and reproducibility (8). Although clinical performance data are summarized from the Potter (4) and Johnson (5) publications, the SSED does not cite those publications or provide detail about possible FDA supervision or review of the Potter study (e.g., about how blinding may have been assured in a post hoc analysis). Nor does the SSED discuss how well the FDA’s adherence question may have been addressed by Liles (7). This lack of clarity is striking because the FDA’s instruction template provided to sponsors writing a SSED states to ‘Describe any information submitted by the applicant in response to outstanding issues, and whether the response was found acceptable’ (9).” (Ransohoff, 2020).
The author concluded his answer with “Although the word “effectiveness” commonly refers to long-term benefits and harms (12), the word when used by the FDA in evaluating a test may refer to test discrimination: “. . .analyses of effectiveness based on sensitivity and specificity” [(8), page 27]. Although FDA “approval” carries great weight, the implications of that approval are limited.”
We agree with the author in that the concerns from the FDA about the 20% false positive rate were not addressed in the sponsor’s Summary of Safety and Effectiveness Data (SSED) and not answered in the Liles (2017) study. We acknowledge that the FDA approval process addresses analytic validity and clinical validity, but it does not answer clinical utility, i.e., whether the blood-based screening test improves health outcomes, such as cancer survival, among Medicare beneficiaries.
Second, how does a test with a low degree of discrimination manage to achieve such a high degree of cost-effectiveness in CEA modeling?
“The mSEPT9 test has limited ability to discriminate cancer from no cancer because its positivity rate is 68% in persons with CRC and 20% in persons with no colonic disease. Because the false positive rate is 20%—not 2% or 0.2%—the ratio of false positives to true positives is extraordinarily high: 37.8 false positives per true-positive result compared with 5.4 for FIT [ref (8) page 33], even though the 2 tests have similar sensitivity for CRC [68% for mSEPT9 and 74% for FIT (3)]. Although colonoscopy following a positive mSEPT9 may find adenomas that may be precursors to CRC, mSEPT9 cannot be credited with finding them, because mSEPT9 has the same 20% positivity rate both in persons with no colonic lesions and in persons with even advanced adenomas (4).” (Ransohoff, 2020).
“The way that a test with such a low level of discrimination can be so cost effective in a CEA is simple to understand. A test with a 20% positivity rate when applied yearly [the “most cost effective” strategy among the 4 new tests, according to the CEA (3)] leads to a cumulative positivity rate of 50% at 3 years and 70% at 5 years. Thus, virtually all participants are enrolled in colonoscopy within a few years of receiving yearly mSEPT9. A testing program that soon puts everyone into colonoscopy will necessarily have cost-effectiveness roughly similar to that of colonoscopy…. The mechanism by which chance may result in a positive outcome has been called “serendipity” and is not new in the example of mSEPT9. For mSEPT9, however, the magnitude of the mechanism is dramatic because its false-positive rate is so high.” (Ransohoff, 2020).
We acknowledge the author’s conclusion that “In sum, although the mSEPT9 test is technically cost effective, it achieves cost-effectiveness by an unusual mechanism—a high false-positive rate that causes people, by chance, to become enrolled in colonoscopy screening.”
Third, what important unintended consequences may arise as a result of upcoming policy determinations about mSEPT9 by CMS and USPSTF?
“For doctors and patients, the implications of endorsing a screening strategy that operates by “chance” would be relatively straightforward to address, if perhaps a bit awkward. Doctors could explain to patients that using the test on a yearly basis would result in a 50% chance of having a colonoscopy within 3 years and 70% within 5 years, so that using the test is at best buying a small amount of time before colonoscopy is conducted.“ (Ransohoff, 2020).
“For policy makers such as the CMS and USPSTF, the implications are more dramatic. Is this the mechanism that we, as policy makers, want to use to get people to have a colonoscopy— that is, by practically “tricking” them because of a false-positive test result? There is something unsettling about this logic….A further consequence—unusual, unintended, and potentially important—may be the impact of mSEPT9 adoption on test developers like academic laboratories and companies. If a screening test can be successful and adopted because of its high false-positive rate, then why not simply lower the cutoff levels of existing tests such as FIT or mtSDNA or of the next new noninvasive test for CRC so that greater numbers of people are recommended to have colonoscopy? That interpretation could have a chilling effect on efforts to develop screening tests that actually achieve a high degree of discrimination. At an extreme, a test developer could see its goal as to create a test with a high positivity rate that people “believe in” and so, for example as in this instance, will receive colonoscopy if the test is positive. Are these the precedents that policy makers like CMS and USPSTF want to encourage?” (Ransohoff, 2020).
We acknowledge the author’s conclusion that “Because approval decisions of leading policy-making institutions like the FDA, CMS, and USPSTF are so influential, their determinations must be clearly described and explained, including consideration of possible unintended consequences.” (Ransohoff,
2020).
Thus, we strive for transparency in the policy decision making process, and want to balance the tradeoffs between the benefits and harms of blood-based colorectal cancer screening tests in the decision memo.
Analysis of the Need for Higher Adherence by Ladabaum (2013)
The purpose of the Ladabaum (2013) study was to conduct “a cost-utility analysis using a validated decision analytic model comparing mSEPT9, fecal occult blood testing (FOBT), fecal immunochemical testing (FIT), sigmoidoscopy, and colonoscopy, projecting lifetime benefits and costs” (Ladabaum, 2013). The authors “modeled the contemporary population in the United States at average risk for colorectal cancer, with age specific all-cause mortality based on U.S. Life Tables from 2003” (Ladabaum, 2013). Screening was superimposed on the Natural History module. In the base case, the authors modeled perfect uptake and adherence, and considered multiple levels of imperfect uptake and adherence in sensitivity analyses. The model was calibrated to Surveillance, Epidemiology, and End Result (SEER) data on stage distribution by localized, regional, and disseminated colorectal cancer. They conducted analyses reflecting persons who take up and adhere with screening and follow-up colonoscopy after abnormal screening (maximum efficacy), as well as scenarios reflecting imperfect uptake, per-cycle adherence, and follow-up (potential effectiveness).
For the overall results, “All established screening strategies were more effective than mSEPT9. FIT was cost saving, dominated mSEPT9, and was preferred among all the alternatives” (Ladabaum, 2013). For example, “Assuming perfect uptake, adherence, and follow-up after abnormal screening, the greatest reductions in colorectal cancer incidence and mortality compared with no screening were observed with sigmoidoscopy/FIT, and the reductions with mSEPT9-3-well and mSEPT9-2-well were lower than with the alternatives….mSEPT9-3well and mSEPT9-2well gained fewer QALYs than the other strategies, and incurred the highest costs (Fig. 1, Table 1)…. [A]nnual FIT was preferred in incremental comparisons between strategies. It was more effective and less costly than mSEPT9-2 well, mSEPT9-3 well, FOBT, sigmoidoscopy, and colonoscopy” (Ladabaum, 2013).
The authors reported some study limitations. “The degree of independence between individual tests in a given strategy is not known, and our model assumes independence. For instance, although improvements in mSEPT9 test-performance with 3 wells compared with 2 wells suggest that additional testing provides incremental yield, the true degree of independence between tests from year to year is not known. However, the effect of assuming independence is likely to be most pronounced for strategies with yearly
testing, including FOBT, which was the subject of one of our encouraging validation exercises (Supplementary Appendix). We did not model adenoma multiplicity or location, and the number of people with adenomas and colorectal cancer detected by size and stage were not validated in the same way that colorectal cancer incidence and mortality reduction were validated (Supplementary Appendix). Disutilities associated with screening are not included; considering modest disutilities for 1 to 2 days every 1 to 10 years does not affect the results substantially (results not shown). In the real world, screening uptake, adherence, and follow-up are complex at the population and individual level. Instead of pure subpopulations, there is likely a distribution of screening behaviors that may vary over time. The data to inform a model with such complex attributes are not currently available” (Ladabaum, 2013).
The authors concluded that “To be cost effective compared with established strategies, mSEPT9 or blood-based biomarkers with similar test performance characteristics would need to achieve substantially higher uptake and adherence rates than the alternatives. It remains to be proven whether colorectal cancer screening with a blood test can improve screening uptake or long-term adherence compared with established strategies” (Ladabaum, 2013).
Analysis of Screening Prevalence from BRFSS
As reported in the Background section of this decision memo, the Centers for Disease Prevention and Control reports CRC screening rates based upon results of the Behavioral Risk Factor Surveillance System. In 2018, the CRC screening test use was 63.3% for individuals aged 50-64 years and 79.2% for individuals aged 65-75 years (overall 68.8%; Joseph et al., 2020 at https://www.cdc.gov/mmwr/volumes/69/wr/mm6910a1.htm, accessed 07/26/2020). Screening data was collected by the Behavioral Risk Factor Surveillance System (BRFSS), which “is an annual, state-based, random-digit–dialed telephone survey of the civilian, noninstitutionalized adult population aged ≥18 years that collects information on health risk behaviors, preventive health practices, and health care access in the United States” (Joseph, 2020). However, “The findings in this report are subject to at least three limitations. First, CRC screening prevalence might be overestimated because BRFSS does not specify whether tests were done for screening or diagnostic purposes. Second, data are self-reported and not validated by medical record review. Third, response rates were low (49.9%), although the BRFSS weighting procedure accounts for nonresponse, and 7.2% of all respondents did not answer all of the questions and were excluded from the analysis.”
While we acknowledge the limitations of the BRFSS which has the potential to overestimate CRC screening prevalence, we believe that the results are likely to be generalizable to the Medicare population since data was collected from all 50 states and is likely to be representative of the US population, in addition to the analysis being stratified by age group 65 to 75 years old.
Analysis of Advanced Adenomas
We reviewed the evidence on the accuracy of non invasive screening tests to detect advanced adenomas. Reporting on stool-based tests in their 2020 draft recommendation statement on colorectal cancer screening, the USPSTF found that the test performance characteristics for FIT were “Similar to HSgFOBT [high-sensitivity guaiac-based fecal occult blood test], [in that] sensitivity for detecting advanced adenomas was lower while specificity was similar; pooled sensitivity was 0.23 (95% CI, 0.20 to 0.25) and pooled specificity was 0.96 (95% CI, 0.95 to 0.97)….In four studies (n=12,424) reporting the accuracy of sDNA-FIT, pooled sensitivity for colorectal cancer detection was 0.93 (95% CI, 0.87 to 1.0) and pooled specificity was 0.84 (95% CI, 0.84 to 0.86), with a lower pooled sensitivity for detecting advanced adenomas (0.43 [95% CI, 0.40 to 0.46]) but higher pooled specificity (0.89 [95% CI, 0.86 to 0.92])” (USPSTF, Draft Recommendation, 2020).
In the evidence review for the 2020 draft recommendation, the USPSTF reported that “based on one fair-quality nested case-control study (n=6857)” (Potter, 2014), one serum test—Epi proColon (Epigenomics, Germantown, MD)— had a sensitivity and specificity to detect advanced adenoma of 0.22 (95% CI, 0.18 to 0.24) and 0.79 (95% CI, 0.76 to 0.82), respectively (Lin, 2020). We included the Potter (2014) study in our internal technology evidence review.
For adults ages 50 to 75 years, the USPSTF concluded that there was “convincing evidence that screening for colorectal cancer with several different methods can accurately detect early-stage colorectal cancer and adenomatous polyps” (USPSTF, Draft Recommendation, 2020).
Several publications submitted with the public comments discuss the benefits of screening for advanced adenomas. The Corley (2014) observational study found that “The adenoma detection rate [based on colonoscopies) was inversely associated with the risks of interval colorectal cancer, advanced-stage interval cancer, and fatal interval cancer.” The authors defined the adenoma detection rate as the proportion of screening colonoscopies performed by a physician that detect at least one histologically confirmed colorectal adenoma or adenocarcinoma.
In the Crotta (2012) prospective cohort study of 2959 average risk individuals evaluated over four screening rounds with FIT in population-based screening program, the authors concluded that ” A high detection rate of advanced adenomas in all rounds indicates that FIT screening could have a higher impact on incidence of CRC than the guaiac fecal occult blood test.”
Simulation modeling studies also demonstrated benefit for detecting advanced adenomas. The Haug (2015) study used the Simulation Model of Colorectal Cancer (SimCRC) to determine that “Screening with the NIT [a new hypothetical non-invasive test] was not more effective, but was 29–44% more costly than screening with FOBTs….A comparative modelling approach using a model that assumes a shorter adenoma dwell time (MISCAN-COLON) confirmed the superiority of the immunochemical FOBT over a NIT with no ability to detect adenomas.” The authors concluded that “information on adenoma detection is crucial to determine whether a new NIT is a viable alternative to FOBTs for CRC screening. Studies that aim at developing alternatives to FOBTs for optimizing CRC screening should therefore pay special attention to the detection of adenomas in addition to the detection of CRC” (Haug, 2015). In the microsimulation modeling study by Meester et al. (2015), the authors concluded that “higher adenoma detection was associated with lower lifetime colorectal cancer incidence and mortality without higher overall costs. Future research is needed to assess if increasing adenoma detection would be associated with improved patient outcomes” (Meester, 2015).
In the editorial by Lieberman (2020) on colon polyp surveillance after polypectomy, the authors believe that “While we await clinical trial information, we should focus our surveillance energy and resources to achieve adherence in the high-risk adenoma (HRA) group, which represents 5% to 10% of patients undergoing screening colonoscopy. We also should focus on colonoscopy quality, which means measuring quality in our endoscopic practice, and striving to improve. These 2 efforts may have a significant potential impact on reducing the risk of postcolonoscopy colorectal cancer (PC-CRC) for our patients” (Lieberman, 2020).
However, there are limitations to screening for advanced adenomas. In the Imperiale (2019) meta analysis of 31 studies using 18 different FITs (120 255 participants), the authors reported that using FIT “For advanced adenomas, sensitivity was 0.40 (CI, 0.33 to 0.47) …at 10 μg/g, and specificity was 0.95 (CI, 0.94 to 0.96)…at greater than 20 μg/g.” Mean age ranged from 48.2 to 64 years. The authors concluded that “Sensitivity of 1-time testing [with FIT] for advanced adenomas is low, regardless of the threshold.” (Imperiale, 2019).
While we acknowledge the utility and potential clinical benefit of screening for advanced adenomas, there is very limited available evidence on the accuracy of blood-based tests to detect advanced adenomas and the sensitivity of FIT for advanced adenoma is low (Imperiale, 2019). Thus, we did not include point sensitivity or specificity to screen for advanced adenoma in the decision.
Conclusions
To assess the performance of a new screening test to detect CRC in this NCA, we specified the threshold of the test performance characteristics of the blood-based CRC screening test to that of existing screening tests, FIT and stool DNA test, in the intended use setting. Thus, if the sensitivity and specificity of the new screening test is as good as, ideally better than, the point sensitivity of FIT and the point specificity of a stool DNA test, then we believe there would be indirect evidence of impact of the blood-based biomarker test that establishes a link to colorectal cancer mortality.
Epi proColon®
The published studies show the sensitivity of the Epi proColon® test to be no better than FIT in detection of colorectal cancer. Compared to the FIT test, the specificity for Epi proColon® was lower. The published evidence does not demonstrate that using Epi proColon® prevents more cancers or improves survival for Medicare patients. The Epi proColon® test performance does not meet sensitivity and specificity levels established by prior evidence at which the benefits of using the screening test outweigh harms to Medicare patients.
Health Disparities
Colorectal cancer disproportionately affects adults 50 years of age and older, with the highest death rate among people aged 75-84 years. (NIH/SEER 2020). African-Americans have the highest death rate compared to other races (NIH/SEER 2020). Enrollment of adults older than 70 years in the study by Potter (2014) was specifically enhanced to increase generalizability to the Medicare population, and enrolled representative samples of nonwhites while still balanced for gender based on United States
census data. Both genders were adequately represented in the evidence base. Four studies (Johnson, 2014; Potter, 2014; Song, Jia, Yu, 2017; Song Peng, Li, 2017) included African Americans in their study populations. Given the burden of CRC, CMS encourages all eligible Medicare beneficiaries to participate in CRC screening.
Summary
To assess the performance of a new screening test to prevent and detect CRC, direct high strength evidence that using the test improves health outcomes would be important. We recognized the need for innovation in cancer screening and have also included indirect evidence from appropriate studies on test performance in past NCDs. We determined the performance threshold based on evidence for cancer prevention and early detection. At this time, direct evidence only exists for stool-based non-invasive screening tests with FIT being the most widely available and appropriate option. Accordingly, if the sensitivity and specificity of the new screening test is as good as or better than the point sensitivity of FIT and the point specificity of a stool DNA test, then we believe we would have indirect evidence of impact of the blood-based biomarker test that establishes a link to colorectal cancer mortality.
Based on the published studies and evidence, the Epi proColon® does not meet test or coverage criteria. Overall, we find that the published evidence does not demonstrate that screening for colorectal cancer with the blood-based Epi proColon® test will improve health outcomes for the Medicare population.
To foster innovation, we believe it is important to rapidly provide coverage of CRC screening tests that meet patient and test criteria and will cover these appropriate CRC screening tests immediately without having to reconsider this NCD. We believe this will provide a clear path to national Medicare coverage, increase access to appropriate screening tests and reduce burden on manufacturers, providers and patients.
IX. Conclusion
The Centers for Medicare & Medicaid Services (CMS) has determined that the evidence is sufficient to cover a blood-based biomarker test as an appropriate colorectal cancer screening test once every 3 years for Medicare beneficiaries when performed in a Clinical Laboratory Improvement Act (CLIA)-certified laboratory, when ordered by a treating physician and when all of the following requirements are met:
The patient is:
- age 50-85 years, and,
- asymptomatic (no signs or symptoms of colorectal disease including but not limited to lower gastrointestinal pain, blood in stool, positive guaiac fecal occult blood test or fecal immunochemical test), and,
- at average risk of developing colorectal cancer (no personal history of adenomatous polyps, colorectal cancer, or inflammatory bowel disease, including Crohn’s Disease and ulcerative colitis; no family history of colorectal cancers or adenomatous polyps, familial adenomatous polyposis, or hereditary nonpolyposis colorectal cancer).
The blood-based biomarker screening test must have all of the following:
- FDA market authorization with an indication for colorectal cancer screening; and
- proven test performance characteristics for a blood-based screening test with both sensitivity greater than or equal to 74% and specificity greater than or equal to 90% in the detection of colorectal cancer compared to the recognized standard (accepted as colonoscopy at this time), based on the pivotal studies included in the FDA labeling.
The currently available Epi proColon® test does not meet the criteria for an appropriate blood-based biomarker CRC screening test. Based on the evidence at this time, we will non-cover the Epi proColon® test.
See Appendix B for the draft manual language.
APPENDIX A
General Methodological Principles of Study
Design
(Section VI of the Decision Memorandum)
When making national coverage determinations, CMS evaluates relevant clinical evidence to determine whether or not the evidence is of sufficient quality to support a finding that an item or service is reasonable and necessary. The overall objective for the critical appraisal of the evidence is to determine to what degree we are confident that: 1) the specific assessment questions can be answered conclusively; and 2) the intervention will improve health outcomes for patients.
We divide the assessment of clinical evidence into three stages: 1) the quality of the individual studies; 2) the generalizability of findings from individual studies to the Medicare population; and 3) overarching conclusions that can be drawn from the body of the evidence on the direction and magnitude of the intervention’s potential risks and benefits.
The methodological principles described below represent a broad discussion of the issues we consider when reviewing clinical evidence. However, it should be noted that each coverage determination has its unique methodological aspects.
Assessing Individual Studies
Methodologists have developed criteria to determine weaknesses and strengths of clinical research. Strength of evidence generally refers to: 1) the scientific validity underlying study findings regarding causal relationships between health care interventions and health outcomes; and 2) the reduction of bias. In general, some of the methodological attributes associated with stronger evidence include those listed below:
- Use of randomization (allocation of patients to either intervention or control group) in order to minimize bias.
- Use of contemporaneous control groups (rather than historical controls) in order to ensure comparability between the intervention and control groups.
- Prospective (rather than retrospective) studies to ensure a more thorough and systematical assessment of factors related to outcomes.
- Larger sample sizes in studies to demonstrate both statistically significant as well as clinically significant outcomes that can be extrapolated to the Medicare population. Sample size should be large enough to make chance an unlikely explanation for what was found.
- Masking (blinding) to ensure patients and investigators do not know to that group patients were assigned (intervention or control). This is important especially in subjective outcomes, such as pain or quality of life, where enthusiasm and psychological factors may lead to an improved perceived outcome by either the patient or assessor.
Regardless of whether the design of a study is a randomized controlled trial, a non-randomized controlled trial, a cohort study or a case-control study, the primary criterion for methodological strength or quality is to the extent that differences between intervention and control groups can be attributed to the intervention studied. This is known as internal validity. Various types of bias can undermine internal validity. These include:
- Different characteristics between patients participating and those theoretically eligible for study but not participating (selection bias).
- Co-interventions or provision of care apart from the intervention under evaluation (performance bias).
- Differential assessment of outcome (detection bias).
- Occurrence and reporting of patients who do not complete the study (attrition bias).
In principle, rankings of research design have been based on the ability of each study design category to minimize these biases. A randomized controlled trial minimizes systematic bias (in theory) by selecting a sample of participants from a particular population and allocating them randomly to the intervention and control groups. Thus, in general, randomized controlled studies have been typically assigned the greatest strength, followed by non-randomized clinical trials and controlled observational studies. The design, conduct and analysis of trials are important factors as well. For example, a well-designed and conducted observational study with a large sample size may provide stronger evidence than a poorly designed and conducted randomized controlled trial with a small sample size. The following is a representative list of study designs (some of that have alternative names) ranked from most to least methodologically rigorous in their potential ability to minimize systematic bias:
Randomized controlled trials
Non-randomized controlled trials
Prospective cohort studies
Retrospective case control studies
Cross-sectional studies
Surveillance studies (e. g. , using registries or surveys)
Consecutive case series
Single case reports
When there are merely associations but not causal relationships between a study’s variables and outcomes, it is important not to draw causal inferences. Confounding refers to independent variables that systematically vary with the causal variable. This distorts measurement of the outcome of interest because its effect size is mixed with the effects of other extraneous factors. For observational, and in some cases randomized controlled trials, the method in that confounding factors are handled (either through stratification or appropriate statistical modeling) are of particular concern. For example, in order to interpret and generalize conclusions to
our population of Medicare patients, it may be necessary for studies to match or stratify their intervention and control groups by patient age or co-morbidities.
Methodological strength is, therefore, a multidimensional concept that relates to the design, implementation and analysis of a clinical study. In addition, thorough documentation of the conduct of the research, particularly study selection criteria, rate of attrition and process for data collection, is essential for CMS to adequately assess and consider the evidence.
Generalizability of Clinical Evidence to the Medicare Population
The applicability of the results of a study to other populations, settings, treatment regimens and outcomes assessed is known as external validity. Even well-designed and well-conducted trials may not supply the evidence needed if the results of a study are not applicable to the Medicare population. Evidence that provides accurate information about a population or setting not well represented in the Medicare program would be considered but would suffer from limited generalizability.
The extent to that the results of a trial are applicable to other circumstances is often a matter of judgment that depends on specific study characteristics, primarily the patient population studied (age, sex, severity of disease and presence of co-morbidities) and the care setting (primary to tertiary level of care, as well as the experience and specialization of the care provider). Additional relevant variables are treatment regimens (dosage, timing and route of administration), co-interventions or concomitant therapies, and type of outcome and length of follow-up.
The level of care and the experience of the providers in the study are other crucial elements in assessing a study’s external validity. Trial participants in an academic medical center may receive more or different attention than is typically available in non-tertiary settings. For example, an investigator’s lengthy and detailed explanations of the potential benefits of the intervention and/or the use of new equipment provided to the academic center by the study sponsor may raise doubts about the applicability of study findings to community practice.
Given the evidence available in the research literature, some degree of generalization about an intervention’s potential benefits and harms is invariably required in making coverage determinations for the Medicare population. Conditions that assist us in making reasonable generalizations are biologic plausibility, similarities between the populations studied and Medicare patients (age, sex, ethnicity and clinical presentation) and similarities of the intervention studied to those that would be routinely available in community practice.
A study’s selected outcomes are an important consideration in generalizing available clinical evidence to Medicare coverage determinations. One of the goals of our determination process is to assess health outcomes. These outcomes include resultant risks and benefits such as increased or decreased morbidity and mortality. In order to make this determination, it is often necessary to evaluate whether the strength of the evidence is adequate to draw conclusions about the direction and magnitude of each individual outcome relevant to the intervention under study. In addition, it is important that an intervention’s benefits are clinically significant and durable, rather than marginal or short-lived. Generally, an intervention is not reasonable and necessary if its risks outweigh its benefits.
If key health outcomes have not been studied or the direction of clinical effect is inconclusive, we may also evaluate the strength and adequacy of indirect evidence linking intermediate or surrogate outcomes to our outcomes of interest.
Assessing the Relative Magnitude of Risks and Benefits
Generally, an intervention is not reasonable and necessary if its risks outweigh its benefits. Health outcomes are one of several considerations in determining whether an item or service is reasonable and necessary. CMS places greater emphasis on health outcomes actually experienced by patients, such as quality of life, functional status, duration of disability, morbidity and mortality, and less emphasis on outcomes that patients do not directly experience, such as intermediate outcomes, surrogate outcomes, and laboratory or radiographic responses. The direction, magnitude, and consistency of the risks and benefits across studies are also important considerations. Based on the analysis of the strength of the evidence, CMS assesses the relative magnitude of an intervention or technology’s benefits and risk of harm to Medicare beneficiaries.
APPENDIX B
Medicare National Coverage Determinations Manual
This draft NCD is subject to formal revisions and formatting changes prior to the release of the final NCD contractor instructions and publication in the Medicare National Coverage Determinations Manual.
Table of Contents
(Rev.)
NCD 210.3 Colorectal Cancer Screening Tests
Benefit Category
Colorectal Cancer Screening Tests
A. General
Sections 1861(s)(2)(R) and 1861(pp) of the Social Security Act (the Act) and regulations at 42 CFR 410.37 authorize Medicare coverage for screening colorectal cancer tests under Medicare Part B. The statute and regulations authorize the Secretary to add other tests and procedures (and modifications to tests and procedures for colorectal cancer screening) as the Secretary finds appropriate based on consultation with appropriate organizations.
Indications and Limitations of Coverage
B. Nationally Covered Indications
1. Fecal Occult Blood Tests (FOBT) (effective January 1, 2004)
Fecal occult blood tests (FOBTs) are generally divided into two types: immunoassay and guaiac types. Immunoassay (or immunochemical) fecal occult blood tests (iFOBT) use “antibodies directed against human globin epitopes. While most iFOBTs use spatulas to collect stool samples, some use a brush to collect toilet water surrounding the stool. Most iFOBTs require laboratory processing.
Guaiac fecal occult blood tests (gFOBT) use a peroxidase reaction to indicate presence of the heme portion of hemoglobin. Guaiac turns blue after oxidation by oxidants or peroxidases in the presence of an oxygen donor such as hydrogen peroxide. Most FOBTs use sticks to collect stool samples and may be developed in a physician’s office or a laboratory. In 1998, Medicare began reimbursement for guaiac FOBTs, but not immunoassay type tests for colorectal cancer screening. Since the fundamental process is similar for other iFOBTs, the Centers for Medicare & Medicaid Services evaluated colorectal cancer screening using immunoassay FOBTs in general.
Effective for dates of service on and after January 1, 2004, Medicare covers one screening FOBT per annum for the early detection of colorectal cancer. This means that Medicare will cover one guaiac-based (gFOBT) or one immunoassay-based (iFOBT) at a frequency of every 12 months; i.e., at least 11 months have passed following the month in which the last covered screening FOBT was performed, for beneficiaries aged 50 years and older. The beneficiary completes the existing gFOBT by taking samples from two different sites of three consecutive stools; the beneficiary completes the iFOBT by taking the appropriate number of stool samples according to the specific manufacturer’s instructions. This screening requires a written order from the beneficiary’s attending physician. (“Attending physician” means a doctor of medicine or osteopathy (as defined in §1861(r)(1) of the Act) who is fully knowledgeable about the beneficiary’s medical condition, and who would be responsible for using the results of any examination performed in the overall management of the beneficiary’s specific medical problem.)
2. The Cologuard™ - Multitarget Stool DNA (sDNA) Test (effective October 9, 2014)
Screening stool or fecal DNA (deoxyribonucleic acid, sDNA) testing detects molecular markers of altered DNA that are contained in the cells shed by colorectal cancer and pre-malignant colorectal epithelial neoplasia into the lumen of the large bowel. Through the use of selective enrichment and amplification techniques, sDNA tests are designed to detect very small amounts of DNA markers to identify colorectal cancer or pre-malignant colorectal neoplasia. The Cologuard™ - multitarget sDNA test is a proprietary in vitro diagnostic device that incorporates both sDNA and fecal immunochemical test techniques and is designed to analyze patients’ stool samples for markers
associated with the presence of colorectal cancer and pre-malignant colorectal neoplasia.
Effective for dates of service on or after October 9, 2014, The Cologuard™ test is covered once every three years for Medicare beneficiaries that meet all of the following criteria:
- Age 50 to 85 years, and
- Asymptomatic (no signs or symptoms of colorectal disease including but not limited to lower gastrointestinal pain, blood in stool, positive guaiac fecal occult blood test (gFOBT) or fecal immunochemical test (iFOBT)), and,
- At average risk of developing colorectal cancer (no personal history of adenomatous polyps, colorectal cancer, or inflammatory bowel disease, including Crohn’s Disease and ulcerative colitis; no family history of colorectal cancers or adenomatous polyps, familial adenomatous polyposis, or hereditary nonpolyposis colorectal cancer).
3. Blood-based Biomarker Tests (effective January XX, 2021)
Blood-based DNA testing detects molecular markers of altered DNA that are contained in the cells shed into the lumen of the large bowel by colorectal cancer and pre-malignant colorectal epithelial neoplasia.
Effective for dates of service on or after effective January XX, 2021, a blood-based biomarker test is covered as an appropriate colorectal cancer screening test once every 3 years for Medicare beneficiaries when performed in a Clinical Laboratory Improvement Act (CLIA)-certified laboratory, when ordered by a treating physician and when all of the following requirements are met:
The patient is:
- age 50-85 years, and,
- asymptomatic (no signs or symptoms of colorectal disease including but not limited to lower gastrointestinal pain, blood in stool, positive guaiac fecal occult blood test or fecal immunochemical test), and,
- at average risk of developing colorectal cancer (no personal history of adenomatous polyps, colorectal cancer, or inflammatory bowel disease, including Crohn’s Disease and ulcerative colitis; no family history of colorectal cancers or adenomatous polyps, familial adenomatous polyposis, or hereditary nonpolyposis colorectal cancer).
The blood-based biomarker screening test must have all of the following:
- FDA market authorization with an indication for colorectal cancer screening; and
- proven test performance characteristics for a blood-based screening test with both sensitivity greater than or equal to 74% and specificity greater than or equal to 90% in the detection of colorectal cancer compared to the recognized standard (accepted as colonoscopy at this time), as minimal threshold levels, based on the pivotal studies included in the FDA labeling.
C. Nationally Non-Covered Indications
All other indications for colorectal cancer screening not otherwise specified in the Act and regulations, or otherwise specified above remain nationally non-covered. Non-coverage specifically includes:
(1) All screening sDNA tests, effective April 28, 2008, through October 8, 2014. Effective for dates of service on or after October 9, 2014, all other screening sDNA tests not otherwise specified above remain nationally non-covered.
(2) Screening computed tomographic colonography (CTC), effective May 12, 2009.
D. Other
N/A
(This NCD last reviewed January 2021.)
APPENDIX C –NCD 210.3 (2014)
NCD 210.3 Colorectal Cancer Screening Tests
(Rev. 183, Issued: 08-06-15; Effective: 10-09-14, Implementation: 09-08-2015- For non-shared MAC edits; 01-04-16 - For all shared system changes.)
Benefit Category
Colorectal Cancer Screening Tests
A. General
Sections 1861(s)(2)(R) and 1861(pp) of the Social Security Act (the Act) and regulations at 42 CFR 410.37 authorize Medicare coverage for screening colorectal cancer tests under Medicare Part B. The statute and regulations authorize the Secretary to add other tests and procedures (and modifications to tests and procedures for colorectal cancer screening) as the Secretary finds appropriate based on consultation with appropriate organizations.
Indications and Limitations of Coverage
B. Nationally Covered Indications
1. Fecal Occult Blood Tests (FOBT) (effective January 1, 2004)
Fecal occult blood tests (FOBTs) are generally divided into two types: immunoassay and guaiac types. Immunoassay (or immunochemical) fecal occult blood tests (iFOBT) use “antibodies directed against human globin epitopes. While most iFOBTs use spatulas to collect stool samples, some use a brush to collect toilet water surrounding the stool. Most iFOBTs require laboratory processing.
Guaiac fecal occult blood tests (gFOBT) use a peroxidase reaction to indicate presence of the heme portion of hemoglobin. Guaiac turns blue after oxidation by oxidants or peroxidases in the presence of an oxygen donor such as hydrogen peroxide. Most FOBTs use sticks to collect stool samples and may be developed in a physician’s office or a laboratory. In 1998, Medicare began reimbursement for guaiac FOBTs, but not immunoassay type tests for colorectal cancer screening. Since the fundamental process is similar for other iFOBTs, the Centers for Medicare & Medicaid Services evaluated colorectal cancer screening using immunoassay FOBTs in general.
Effective for dates of service on and after January 1, 2004, Medicare covers one screening FOBT per annum for the early detection of colorectal cancer. This means that Medicare will cover one guaiac-based (gFOBT) or one immunoassay-based (iFOBT) at a frequency of every 12 months; i.e., at least 11 months have passed following the month in which the last covered screening FOBT was performed, for beneficiaries aged 50 years and older. The beneficiary completes the existing gFOBT by taking samples from two different sites of three consecutive stools; the beneficiary completes the iFOBT by taking the appropriate number of stool samples according to the specific manufacturer’s instructions. This screening requires a written order from the eneficiary’s attending physician. (“Attending physician” means a doctor of medicine or osteopathy (as defined in §1861(r)(1) of the Act) who is fully knowledgeable about the beneficiary’s medical condition, and who would be responsible for using the results of any examination performed in the overall management of the beneficiary’s specific medical problem.)
2. The Cologuard™ - Multitarget Stool DNA (sDNA) Test (effective October 9, 2014)
Screening stool or fecal DNA (deoxyribonucleic acid, sDNA) testing detects molecular markers of altered DNA that are contained in the cells shed by colorectal cancer and pre-malignant colorectal epithelial neoplasia into the lumen of the large bowel. Through the use of selective enrichment and amplification techniques, sDNA tests are designed to detect very small amounts of DNA markers to identify colorectal cancer or pre-malignant colorectal neoplasia. The Cologuard™ - multitarget sDNA test is a proprietary in vitro diagnostic device that incorporates both sDNA and fecal immunochemical test techniques and is designed to analyze patients’ stool samples for markers associated with the presence of colorectal cancer and pre-malignant colorectal neoplasia.
Effective for dates of service on or after October 9, 2014, The Cologuard™ test is covered once every three years for Medicare beneficiaries that meet all of the following criteria:
- Age 50 to 85 years, and,
- Asymptomatic (no signs or symptoms of colorectal disease including but not limited to lower gastrointestinal pain, blood in stool, positive guaiac fecal occult blood test (gFOBT) or fecal immunochemical test (iFOBT)), and,
- At average risk of developing colorectal cancer (no personal history of adenomatous polyps, colorectal cancer, or inflammatory bowel disease, including Crohn’s Disease and ulcerative colitis; no family history of colorectal cancers or adenomatous polyps, familial adenomatous polyposis, or hereditary nonpolyposis colorectal cancer).
C. Nationally Non-Covered Indications
All other indications for colorectal cancer screening not otherwise specified in the Act and regulations, or otherwise specified above remain nationally non-covered. Non-coverage specifically includes:
(1) All screening sDNA tests, effective April 28, 2008, through October 8, 2014. Effective for dates of service on or after October 9, 2014, all other screening sDNA tests not otherwise specified above remain nationally non-covered.
(2) Screening computed tomographic colonography (CTC), effective May 12, 2009.
D. Other
N/A
(This NCD last reviewed October 2014.)
Appendix
D
Table 4a is a full table of the sensitivity and specificity of all of the comparative studies found in our internal technology assessment.
| Table 4a. Sensitivity and Specificity of Comparison Studies |
|
Sensitivity (95% CI), % |
P value |
Specificity (95% CI), %, |
P value |
|
Colorectal cancer |
Advanced adenoma-precancerous lesions |
|
Colorectal cancer free |
|
Church, 2014 |
|
|
|
|
|
| Epi proColon® |
48.2 (32.4- 63.6) |
11.2 (7.2-15.7)
(n=314) |
|
91.5 (89.7-93.1) |
|
He, 2018 |
|
|
|
|
|
| Epi proColon® 2.0 |
73.7 |
|
|
97.0 |
|
Hitchins, 2019 |
|
|
|
|
|
| Epi proColon® 2.0 |
70.0 (48-88) |
|
|
100 (89-100) |
|
Jin, 2015 |
|
|
|
|
|
| Epi proColon® 2.0 |
74.8 (67.0–81.6)
(n=135) |
27.4 (18.7–37.6) |
|
87.4 (83.5–90.6)
(n=341) |
|
| FIT (paired with Epi proColon®) |
58.0 (46.1–69.2) (p = 0.03) (n=69 CRC that underwent both FIT and mSEPT9 tests) |
26.9 (p= 0.774) (n = 177) |
|
82.4 (74.4–88.7) (p value not reported)
(n= 108?; non CRC [17769] that underwent both tests) |
|
| Epi proColon® (paired with IT) |
76.8 |
26.9 |
|
|
|
Johnson, 2014 |
|
|
|
|
|
| Epi proColon® |
72.2 (62.5–80.1) |
|
> 0.05 |
80.8 (74.7-85.8) |
< 0.05 |
| FIT |
68.0 (58.2–76.5) (n=97) |
|
|
97.4 (94.1-98.9) (n=193) |
|
Ørntoft, 2015 |
|
|
|
|
|
| Epi proColon® (1/3) |
73 (64–80) |
|
|
82 (75–88) |
|
| Epi proColon® (2/3) |
59 (50–67) |
|
|
95 (91–98) |
|
Potter, 2014 |
|
|
|
|
|
| Epi proColon® |
68 (53–80) |
22 (18–24)
(n=621) |
|
80.0 (78–82) |
|
Song, Peng, Li, 2017 |
|
|
|
|
|
| Epi proColon® 2.0 |
87.1 |
47.0 (without high grade dysplasia)
62.2 (with high grade dysplasia)
(n=148) |
|
|
|
Song, Jia, Yu, 2017 |
|
|
|
|
|
| Epi proColon® 2.0 |
82 |
36
(n=139) |
|
|
|
Song, 2016 |
|
|
|
|
|
| Epi proColon® 2.0 |
|
|
|
|
|
| 1/3 algorithm* |
82.4 |
|
|
82.0 |
|
| 2/3 algorithm+ |
75.1 |
|
|
97.1 |
|
| 1/1 algorithm |
71.3 |
|
|
92.7 |
|
Song, 2018 |
|
|
|
|
|
| Epi proColon® 2.0 |
|
|
|
|
|
| Stage II cancer |
80.6 |
|
|
|
|
| Stage III cancer |
77.4 |
|
|
|
|
| Stage IV cancer |
84.2 |
|
|
|
|
Sun, 2019 |
|
|
|
|
|
| Epi proColon® 2.0 |
73.0 (60.1-83.1) (n=63) |
|
|
94.5 (92.0-96.3) (n=not reported) |
|
| FOBT |
58.7 (45.6–70.8) |
|
|
91.9 (89.0-94.1) |
|
Tóth, 2012 |
|
|
|
|
|
| Epi proColon® 2.0
(1/3)*
(2/3)+ |
95.6 (89.2-98.8)
79.3 (69.6-87.1)
(n=92) |
|
|
84.8 (75.8- 91.4)
99 (94.1-100) (n=92) |
|
| gFOBT |
68.2 (45.1-86.1)
(n=22) |
|
|
70.6 (44 to 89.7)
(n=17) |
|
Warren, 2011 |
|
|
|
|
|
| Epi proColon® |
90.0 (77.4-96.3) |
|
|
88.4 (79.6- 93.7) |
|
*1/3 = a final positive test result if there is one positive count out of three repeat assay runs (1/3 algorithm)
+2/3 = a final positive test result if there was at least two positive counts out of three repeat assay runs (2/3 algorithm)
Appendix E- Supplemental Bibliography
(References submitted through Public Comments/Reviewed but not included in Analysis)
Brenner et al. Risk of progression of advanced adenomas to colorectal cancer by age and sex: estimates based on 840 149 screening colonoscopies Gut. 56(11)1585 (2007).
Brouwers MC, Kerkvliet K, Spithoff K, Consortium ANS. The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. Bmj. 2016;352: i1152.
Chubak J, Garcia MP, Burnett-Hartman AN, et al. Time to colonoscopy after positive fecal blood test in four U.S. health care systems. Cancer Epidemiology Biomarkers and Prevention. 2016;25(2):344-350. doi:10.1158/1055-9965.EPI-15-0470
Clarke, C. A., et al., Projected Reductions in Absolute Cancer–Related Deaths from Diagnosing Cancers Before Metastasis, 2006–2015. Cancer Epidemiology Biomarkers & Prevention. May 2020. Available at: https://cebp.aacrjournals.org/content/29/5/895?iss=5#sec-13
Colditz, G. A., Hoaglin, D. C., & Berkey, C. S. (1997). Cancer incidence and mortality: The priority of screening frequency and population coverage. The Milbank Quarterly, 75(2), 147–173. https://doi.org/10.1111/1468-0009.00050
Collins JF, Lieberman DA, Durbin TE, Weiss DG. Accuracy of screening for fecal occult blood on a single stool sample obtained by digital rectal examination: a comparison with recommended sampling practice. Ann Intern Med. 2005;142: 81-85.
de Moor JS, Cohen RA, Shapiro JA, et al. Colorectal cancer screening in the United States: Trends from 2008 to 2015 and variation by health insurance coverage. Prev Med 2018;112:199-206.
Domanico M, Kisiel J, Gagrat Z, et al. ACG 2019 Annual Scientific Meeting2019 | eventScribe Itinerary Planner. Accessed November 9, 2020. https://www.eventscribe.com/2019/ACG-Abstracts/Presinfo/PresInfo.asp?pres=594316
Doubeni CA, Fedewa SA, Levin TR, et al. Modifiable Failures in the Colorectal Cancer Screening Process and Their Association With Risk of Death. Gastroenterology. 2019;156(1):63-74.e6. doi:10.1053/j.gastro.2018.09.040
Ebner DW, Kisiel JB. Stool-Based Tests for Colorectal Cancer Screening: Performance Benchmarks Lead to High Expected Efficacy. Current Gastroenterology Reports. 2020;22(7). doi:10.1007/s11894-020-00770-6
Gupta and Lieberman. Screening and Surveillance Colonoscopy and COVID-19: Avoiding More Casualties. Gastroenterology. 159, 1205 (2020).
Gupta et al. Recommendations for Follow-Up After Colonoscopy and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer Gastroenterology 158, 1131 (2020).
Hannahan and Folkman. Patterns and Emerging Mechanisms: Review of the Angiogenic Switch during Tumorigenesis. Cell. 86, 353 (1996).
Hu and Curtis. Looking backward in time to define the chronology of metastasis. Nature Comm. 11, 3213 (2020).
Hu et al. Quantitative evidence for early metastatic seeding in colorectal cancer. Nat Genet. 51, 1113 (2019).
Ladabaum U, Mannalithara A, Brill JV, et al. Contrasting Effectiveness and Cost-Effectiveness of Colorectal Cancer Screening Under Commercial Insurance vs. Medicare. Am J Gastroenterol 2018;113:1836-1847.
Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58: 130-160.
Maia et al. Exosome-Based Cell-Cell Communication in the Tumor Microenvironment Frontiers in Cell and Development Biol 6, 1 (2018).
Mannavola et al. Revisiting the Role of Exosomes in Colorectal Cancer: Where Are We Now? Front Oncol 9, 1 (2019).
Mariotto AB, Enewold L, Zhao J, Zeruto CA, Yabroff KR. Medical care costs associated with cancer survivorship in the United States. Cancer Epidemiol Biomarkers, Prev 2020;29:1304–12.
McCarthy AM, Kim JJ, Beaber EF, et al. Follow-Up of Abnormal Breast and Colorectal Cancer Screening by Race/Ethnicity. American Journal of Preventive Medicine. 2016;51(4):507-512. doi:10.1016/j.amepre.2016.03.017
Meester, RGS, Doubeni, C. A., Zauber, A. G., Goede, S. L., Levin, T. R., Corley, D. A., Jemal, A., & Lansdorp-Vogelaar, I. (2015). Public health impact of achieving 80% colorectal cancer screening rates in the United States by 2018. Cancer, 121(13), 2281–2285. https://doi.org/10.1002/cncr.29336
Moffet HH, Parker MM, Sarkar U, et al. Adherence to laboratory test requests by patients with diabetes: The diabetes study of Northern California (DISTANCE). American Journal of Managed Care. 2011;17(5):339-344. Accessed November 9, 2020.
Niedermaier et al. Stage-Specific Sensitivity of Fecal Immunochemical Tests for Detecting Colorectal Cancer: Systematic Review and Meta-Analysis. Amer J Gastroenterology. 115, 56 (2020).
Ofman, J MD “The cancer detection rate—a public health approach to early detection” The Cancer Letter, October 2, 2020. Available at https://cancerletter.com/articles/20201002_7/
Paduch. The role of lymphangiogenesis and angiogenesis in tumor metastasis. Cell Oncol. 39, 397 (2016).
Pantel et al. Circulating Epithelial Cells in Patients with Benign Colon Diseases. Clin Chem. 58, 936 (2011).
Parikh and Prasad. Blood-Based Screening for Colon Cancer A Disruptive Innovation or Simply a Disruption? JAMA. 315, 2519 (2016).
Piscitello A, Edwards DK. Estimating the screening-eligible population size, aged 45 to 74, at average risk to develop colorectal cancer in the United States. Cancer Prev Res. 2020;13(5):443-448.
Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on colorectal cancer. Gastrointestinal Endoscopy. 2017;85(1):2-21.e3. doi:10.1016/j.gie.2016.09.025
Ryser et al. Spatial mutation patterns as markers of early colorectal tumor cell mobility 115, 5774 Proc Natl Acad Sci USA (2018).
Seth A. Seabury et al., Quantifying Gains in the War on Cancer Due to Improved Treatment and Earlier Detection, 19 Health Econ. Policy 141-156 (2016), available at https://www.ncbi.nlm.nih.gov/pubmed/31419891.
Shapiro JA, Bobo JK, Church TR, et al. A Comparison of Fecal Immunochemical and High-Sensitivity Guaiac Tests for Colorectal Cancer Screening. American Journal of Gastroenterology. 2017;112(11):1728-1735. doi:10.1038/ajg.2017.285
Sottoriva et al. A Big Bang model of human colorectal tumor growth Nat Genet 47, 209 (2015).
Virostko J, Capasso A, Yankeelov TE, Goodgame B. Recent trends in the age at diagnosis of colorectal cancer in the US national cancer data base, 2004–2015. Cancer 2019;125:3828–35.
Yadav et al. The Biology and Therapeutic Implications of Tumor Dormancy and Reactivation. Frontiers in Oncol. 8, 1 (2018).
Yeh and Ramaswamy, Mechanisms of Cancer Cell Dormancy—Another Hallmark of Cancer? Can Res. 75, 5014 (2015).
Zauber et al. Colonoscopic Polypectomy and Long-Term Prevention of Colorectal-Cancer Deaths NEJM 366, 687 (2012).
Zorzi, M., et al. (2018). Long-term performance of colorectal cancer screening programmes based on the faecal immunochemical test. Gut, 67(12), 2124–2130. https://doi.org/10.1136/gutjnl-2017-314753


